Introduction
The desire to look good & feel healthy is not limited by age. Today, esthetics is the primary concern of a patient seeking Prosthodontic treatment. For good esthetics, selecting the anterior teeth of correct size, shape & color is salient & for good functional ability, arranging the teeth in correct plane of occlusion is pivotal.
The occlusal plane, lost in patients rendered edentulous, should be relocated if complete dentures are to be aesthetically and functionally satisfactory. The orientation of the occlusal plane forms the basis for teeth arrangement conducive to satisfactory esthetics & proper function. Thus it is one of the most important clinical procedures in prosthodontic rehabilitation.
The GLOSSARY OF PROSTHODONTIC TERMS (July 2005) defines occlusal plane as "the average plane established by the incisal and occlusal surfaces of the teeth". Generally, it is not a plane but represents the planar mean of the curvature of these surfaces. A plane is determined by at least three reference points that are not in a straight line.
Anteriorly, occlusal plane mainly helps in achieving esthetics and phonetics while posteriorly, it forms a milling surface. Thus, incorrect record of the occlusal plane would hamper esthetics, phonetics, and mastication. It may also affect the stability of a complete denture and ultimately result in alveolar bone resorption.
Functionally, the inclination of the occlusal plane is one of the key factors governing occlusal balance. The movement of the mouth during chewing shows a harmonious relationship between the tongue, the mandibular posterior teeth, and the buccinator muscle. The incorrect location of occlusal plane, results in malfunctions. Where the occlusal plane is too high, the tongue and buccinator muscle are not able to position the food bolus on the occlusal plane and hold it there during mastication. There is also a tendency for accumulation of food in the buccal and lingual sulci. An occlusal plane that is too low could lead to tongue and cheek biting.
One of the aims of prosthetic rehabilitation is to restore esthetics. The incisors & canines take on a fundamental role in fulfilling these functions. The amount of visible anterior teeth, with lip at rest or during function, is an important esthetic factor in determining the outcome of prosthodontic care. An acceptable amount of incisal edge display at rest depicts patient’s age.
Accurate determination of occlusal plane is also a pre-requisite for correct phonation. An incorrect occlusal plane can lead to speech difficulties in the form of incorrect pronunciations of certain sounds like ‘f’, ‘v’, ‘s’ etc. This inturn can lead to psychological disturbances in the patient.
Thus, it can be said that, for the success of complete denture prosthesis, arranging the teeth in correct plane of occlusion is pivotal. Changes in the plane of occlusion modify the physical & functional relationship of the oral musculature leading to an alteration in function, comfort & also the esthetic value. Considering the importance of the accurate establishment of the location and the effect of the inclination of the established occlusal plane on function, esthetics and speech, a method to conform it to the occlusal plane that existed in the natural teeth seems necessary.
Many authors have suggested the use of pre-extraction records like pre-extraction diagnostic casts (PEDCs)[1], instruments (the Dakometer[2], profile template[3], Willis gauge[4], Sorenson profile scale[5], and orofacial device[6]), measurements (between tattoo points[7], of the closest speaking space[8], and of the physiological rest position[9]), photographs[10], and radiographs[11]. The review of the literature indicated that PERs provided a useful guide in determining the edentulous patient’s original VDO and arranging the maxillary anterior teeth[12].
In the maxilla, the incisive papilla is a stable anatomic landmark[13] and it can be used to determine the edentulous patient’s vertical relation. Unfortunately, there is no stable anatomic landmark in the mandible.
The purpose of this study was to evaluate the reliability of the measurement of the distance between the lingual frenum and the incisal edges of the mandibular central incisor & the labial frenum and the incisal edges of the mandibular central incisor as pre-extraction records for determining the vertical position of the mandibular incisors in complete dentures.
Aims & Objectives
1. To measure the distance between the mandibular labial frenum & incisal edge of mandibular central incisors so as to evaluate its importance for determining the plane of occlusion.
2. To evaluate the accuracy of distance between lingual frenum & incisal edges of mandibular incisors as pre – extraction record for determining the plane of occlusion.
3. To compare the accuracy of labial & lingual frenum for determining the occlusal plane in Angle’s class I, II & III subjects
Review Of Literature
Numerous authors have advocated different methods for the orientation of the occlusal plane. Most important & accurate of these is pre-extraction record, eg: profile photographs, lead wire, acrylic face mask, dentulous casts etc. Unfortunately, these records are generally not available. P. F. Foley & G. H. Latta[14] through their study determined that there is a fairly constant relationship between the parotid papilla and the occlusal plane. An additional finding was that this relationship may not be the same on each side of the mouth. Race and sex differences were not significant. Majid Bissasu,1999[15] used the location of lingual frenum in determining the original vertical position of mandibular anterior teeth. He concluded that when recorded during function, lingual frenum is a relatively stable landmark. J. Mamootil (1994)[16] gave a new concept of the plane of occlusion based on anatomical landmarks. The posterior end of the plane was set by the centres of the retromolar pads, and the anterior end of the plane was at the upper lip line. Sheldon Winkler (2000)[17] said that the maxillary occlusal rim in anterior region should be 1 - 2mm below the relaxed lip. For the mandibular rim the mandibular lower canine & 1st premolar should lie at or very near the commissure of the lips at rest. J. F. McCord and A. A. Grant (2000)[18] in their article says that ideally, the incisal level of the upper rim is 2 mm inferior to the resting upper lip; the clinician should temper this by deciding what is appropriate for each patient. In younger patients it may 4–5 mm beneath the resting lip, In a old patient it might at level with the resting lip, or possibly 1 mm above this. Donald F. Reikie (2001)[19] said that stable occlusal plane can be correlated with the desired incisal display with lips at rest (generally averaging 2 mm in males and 3.5 mm in females and decreasing with age). Ideally, 1 to 1.5 mm of mandibular incisal length is visible when lips are at rest (repose), The clinically established ideal maxillary central incisor position allows to establish the optimum posterior occlusal plane. K.-H Utz & F. Muller et al (2004)[20] measured the horizontal and vertical tooth positions of functionally and aesthetically pleasing dentures to pre-shape the rims of functional impression trays in the maxillary and the mandibular jaw. For the maxillary denture, they found the distance from the maxillary incisor to the incisive papilla to be12.7 ± 2.8, from the maxillary molar to the maxillary alveolar ridge to be 8.7 ± 2 .5 & from the top of maxillary flange to the maxillary incisor to be 23.1 ± 2.9. In case of mandibular dentures, the distances were: Mandibular incisor to mandibular alveolar ridge was 12.2 ± 2.7, Mandibular right molar to mandibular alveolar ridge was13 ± 3.4, Level of incisal edges of right mandibular lateral incisor and canine to mandibular flange was 15.1 ± 2.1. K Shigli, B.R.Chetal, J. Jabade[21] studied the relation of various soft tissue landmarks like retromolar pad, parotid papilla, commissure of the lips, buccinator groove etc. to the occlusal plane. They found that: the mean values of all readings of buccinator groove was 0.94 mm below the mandibular occlusal plane & the commissure of the lip was inferior to the mandibular occlusal plane by 1.37 mm. Irfan Ahmad (2005)[22] in his article on anterior esthetics said that there are two lip positions: static (at rest) & dynamic (smile). He studied the maxillary lip length in relation to anterior tooth exposure. He said that for a short lip length of 10 – 15mm, the exposure of maxillary central incisor is 3.92mm while for mandibular central is 0.64mm, for a medium lip of 16 – 20mm; they are 3.44mm & 0.77mm respectively. For a long lip (26 – 30mm) the maxillary incisor shows about 0.93mm & mandibular incisor shows 1.95mm.
It is evident that the various concepts reported in the literature allow variation in the location of occlusal plane. But, pre-extraction records remain the most important & accurate of these concepts.
Material And Methods
The study was carried out on 90 completely dentulous patients between the age group of 20 – 35 yrs. The subjects were selected & divided into three groups on the basis of the Angles class I, II & III.
Selection Criteria
The selected subjects showed all healthy permanent incisors with no gingival or periodontal conditions or therapy that would undermine a healthy tooth-to-tissue relationship.
Subjects with Abraded or attrited incisors, Ankyloglossia, Restorations that grossly altered the height of central incisors, Periodontally compromised or supraerupted teeth were rejected. There was no history of Orthodontic treatment or any Facial trauma or surgery
 | Fig - 1
 |
 | Fig -2
|
 | Fig -3
|
 | Fig -4
|
 | Table 1
|
Procedure
The subjects were selected & divided into three groups on the basis of ANGEL’S class I, II & III. Three impressions of the mandibular arch of each patient were made with irreversible hydrocolloid impression material (alginate – Zelgan 2002.Dentsply). Both the labial & lingual frenii were recorded in their functional position. The labial frenum was recorded by pulling the lower lip upwards & outwards. The lingual frenum was recorded by asking the subject to touch the posterior part of the hard palate with his tongue.
The impressions were poured in class III dental stone (Kalstone). The bases were poured in class II type of plaster of paris (Fig.: 1). The cast was then mounted on Ney surveyor (Dentsply). The tilt was adjusted such that the analyzing rod touches the
alveolar attachment of the labial frenum & the anterior attachment of the lingual frenum at the same inclination (Fig.: 2). Tripodization of the cast was then done.
The analyzing rod was then placed at the labial frenum & the level of the incisal surface of the mandibular central incisors was then marked on the analyzing rod using a permanent marker (Fig.: 3). Digital vernier calipers, with an accuracy of .001mm, were used to check the distance between the tip of the analyzing rod & the mark on the rod. This distance was recorded (Fig.: 4). Similar procedure was then carried out for the lingual frenum.
 | Fig -6
|
 | Fig -7
|
Same procedure was then repeated on the rest of the two casts of the subject. The mean & standard deviation of the three readings was calculated & statistically analyzed.
Results
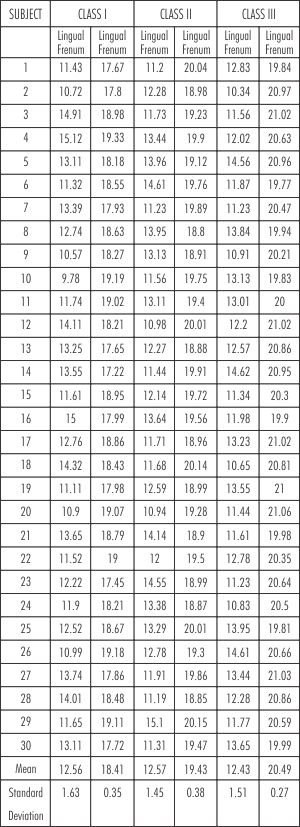
The means and Standard Deviation of all the subjects are presented in (Table I). The Standard Deviation on labial frenum in class I, II & III subjects is quite high i.e. 1.63, 1.45 & 1.51mm respectively (Fig.: 5). Hence, labial frenum cannot be considered as a reliable pre-extraction record landmark. This is further supported by the t-test results which revealed that the relationship of labial frenum in the three classes is almost same & hence clinically insignificant.
The Standard Deviation on lingual frenum in class I, II & III subjects is low i.e. 0.35, 0.38 & 0.27mm respectively (Fig.: 6). Hence, it can be considered as a reliable landmark. This is further supported by the t-test results which revealed that the relationship of lingual frenum is varying, & hence is significant.
Thus, this study revealed that the standard deviation & coefficient of variance of the distance between the labial frenum & incisal edges of mandibular centrals is quite high, While between that of lingual frenum incisal edges of mandibular incisors is clinically insignificant.
Hence, the lingual frenum can be used as pre-extraction record for the orientation of occlusal plane in complete dentures.
Discussion
Correct registration of vertical dimensions of occlusion is of stellar importance in fabrication of complete dentures. When artificial teeth are set in proper positions, the foundation is correctly laid for natural speech, pleasing appearances, and normal function. Alteration in the dimensions can lead to impaired esthetics, can induce speech difficulties & muscle discomfort.
According to Priest, for prosthesis to be successful, it should basically fulfill four levels of patients needs - first comfort, then function followed by esthetics & lastly self esteem[23]. A person cannot rise to the upper level until the lower level is achieved.
Incorrect location of occlusal plane disturbs the harmonious relationship between the oral & perioral musculature & the teeth. The muscles will not be able to rest against the teeth, resulting in fatigue & discomfort. Hence, the first level of hierarchy is disturbed.
If the occlusal plane is too high, normal chewing is impaired, as the food cannot be properly placed back on the occlusal surfaces by the tongue lingually &
buccinator buccally. If too low, then the tongue & cheek can overlap the lower teeth, causing tongue or cheek biting. Thus, the second level is also disturbed.
The amount of visible anterior teeth, with lip at rest or during function, plays an important role in facial aesthetics. Improper occlusal plane, either in location or inclination, can lead to esthetic problems, disturbing the third level of hierarchy. This also in turn affects the patient’s self-esteem.
Unfortunately, there is no precise method for determining the correct vertical dimensions of occlusion. The various concepts & landmarks reported in the literature by numerous authors for determination of occlusal plane in complete dentures unfortunately allow variations in the orientation. Thus, the only way to record the VDO of an edentulous patient more accurately would be to record the VDO before the extraction of the remaining teeth.
The results of this study indicate that the standard deviation between the anterior attachment of the lingual frenum when recorded during function & the incisal edges of the mandibular teeth is clinically low in all the three classes. On the other hand, the standard deviation between the anterior attachment of the labial frenum when recorded during function & the incisal edges of the mandibular teeth is high in all the three classes. Thus, it can be said that the distance between the labial frenum & the incisal edges of mandibular central incisors is not a reliable guide for determining the position of mandibular anterior teeth while the anterior attachment of the lingual frenum when recorded during function can be used as a reliable pre-extraction record for the orientation of occlusal plane.
The results of this study indicate that the distance between the anterior attachment of the lingual frenum and the incisal edges of mandibular central incisors was reliable when the frenum was recorded during function. Consequently, when measurements are made on pre-extraction diagnostic casts from the anterior attachment of the lingual frenum when recorded during function to the incisal edges of mandibular central incisors, then the vertical height of mandibular wax occlusion rims are adjusted anteriorly to correspond with these measurements. The vertical position of the mandibular incisors can then be copied in the complete dentures. Thus, the VDO of the edentulous patient can be preserved.
Conclusion
Within the limits of this study, it was concluded that:
The distance between the labial frenum & the incisal edges of mandibular central incisors is not a reliable guide for determining the position of mandibular anterior teeth.
The lingual frenum when recorded in function is a relatively stable landmark & hence, can be used as a pre-extraction record for determining the original position of the occlusal plane.
References:
1. Murphy WM. Pre-extraction records in full denture construction. Br Dent J 1964;5:391-5.
2. Turrell AJW. Clinical assessment of vertical dimension. J Prosthet Dent 1972;28:238-46.
3. Crabtree DG, Ward JE, McCasland JP. A pre-extraction profile record. J Prosthet Dent 1981;45:479-83.
4. Willis FM. Features of the face involved in full denture prosthesis. Dent Cosmos 1935;77:851-4.
5. Smith DE. The reliability of pre-extraction records for complete dentures. J Prosthet Dent 1971;25:592-608.
6. Aboul-Ela LM, Razek MKA. Pre-extraction records of occlusal plane and vertical dimension. J Prosthet Dent 1977;38:490-3.
7. Silverman MM. Pre-extraction records to avoid premature aging of the denture patient. J Prosthet Dent 1955;5:465-76.
8. Silverman MM. Speaking method in measuring vertical dimension. J Prosthet Dent 1953;3:193-9.
9. Gillis RR. Establishing vertical dimension in full denture construction. J Am Dent Assoc 1941;28:430-6.
10. Wright WH. Use of intra-oral jaw relation wax records in complete denture prosthesis. J Am Dent Assoc 1939;26:542-5.
11. Sharry JJ. Complete denture prosthodontics. McGraw-Hill; 1974
12. Bissasuv M.: Pre-extraction records for complete denture fabrication: A literature review. J Prosthet Dent 2004;91:55-8
13. Harper RN.: The incisive papilla - the basis of a technic to reproduce the positions of key teeth in prosthodontia. J.D. Res. 1948; 27(6): 661 – 668.
14. Foley PF, Latta GH.: A study of the position of the parotid papilla relative to the occlusal plane. J. Prosthet. Dent. 1985 Jan; 53(1): 124-6.
15. Bissasu M.: Use of lingual frenum in determining the original vertical position of mandibular anterior teeth. J. Prosthet. Dent. 1999; 82: 177-81.
16. Mamootil JA.: Plane of occlusion--a new concept. Aust Dent J. 1994 Oct; 39(5): 306-9.
17. Sheldon Winkler: Essentials of complete denture prosthodontics. Second edition, Ishiyaku EuroAmerica Inc. & AITBS Publishers: 2000.
18. McCord JF. & Grant AA.: Registration: Stage I —Creating and outlining the form of the upper denture. British Dental J. 2000; 188 (10): 529 – 36.
19. Reikie DF.: Orthodontically Assisted Restorative Dentistry. J Can Dent Assoc 2001; 67(9): 516-20.
20. Utz KH., Muller F., Kettner N., Reppert G. & Koeck B.: Functional impression and jaw registration: a single session procedure for the construction of complete dentures. J. Oral Rehab. 2004; 31: 554–561
21. Shigli K, Chetal BR, Jabade J.: Validity of soft tissue landmarks in determining the occlusal plane. J Indian Prosthodont Soc 2005; 5: 139-145.
22. I. Ahmad.: Anterior dental aesthetics: dentofacial perspective. BDJ 2005’ July; 199 (2): 81 – 88.
23. Ronald E. Goldstein: Esthetics in dentistry, second edition, B. C. Decker Inc.: 1998. |