Introduction
The term biofilm was introduced to designate the thin-layered condensations of microbes (e.g. bacteria, fungi, protozoa) that may occur on various surface structures in nature. Free-floating bacteria existing in an aqueous environment, so-called planktonic microorganisms are a prerequisite for biofilm formation. Such films may thus become established on any organic or inorganic surface substrate where planktonic microorganisms prevail in a water-based solution. In dental contexts, a well-known and extensively studied biofilm structure is established during the attachment of bacteria to teeth to form dental plaque. Here, bacteria free in saliva (planktonic organisms) serve as the primary source for the organization of this specific biofilm [1].
As far as endodontic infections are concerned, the biofilm concept has thus far gained limited attention. It has been discussed mainly within the framework of bacterial appearances on root tips of teeth with non-vital pulps [2], [3], [4], [5], [6]. Such bacterial aggregations have been thought to be the cause of therapy-resistant apical periodontitis [6], [7]. Although not described in great detail, bacterial condensations on the walls of infected root canals have been observed [8], [9] suggesting that mechanisms for biofilm formation may also exist inside the root canal space. In fact, biofilms have been experimentally produced in root canals of extracted teeth with mixed cultures of anaerobic bacteria [10] or pure cultures of Enterococcus faecalis [11], [12].
Formation Of Biofilm
Biofilm formation is a step-wise procedure its formation occurs in the presence of microorganisms, fluid and solid surface. The phases for microbial community to develop a biofilm and colonize the environment may sometimes be unusual, but basically occur with the same sequence of developmental steps:
1. Deposition of conditioning film
2. Adhesion and colonization of planktonic microorganisms
3. Bacterial growth and biofilm expansion
4. Detachment of biofilm microorganisms into their surroundings.
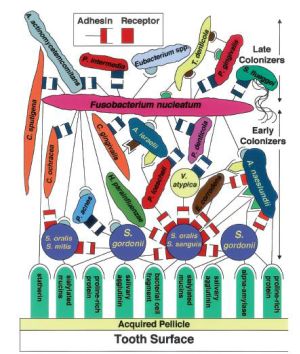
Step 1 involves adsorption of inorganic and organic molecules, to the solid surface which leads to the formation of conditioning film. Conditioning film is composed of proteins and glycoproteins which are derived from saliva and gingival crevicular fluid [13]. Dental plaque formation on the tooth surface involves conditioning with salivary pellicle.
Step 2 involves Adhesion and colonization of planktonic microorganisms and its attachment is strengthened by polymer production and unfolding of cell surface structures. Pioneer organism which is involved in the formation of biofilm on the tooth surface is streptococcus followed by subsequent attachment of gram positive and gram negative bacteria's [14].
There are numerous factors affecting bacterial attachment which includes pH, temperature variations, flow rate of fluid, nutrients, surface energy of the substrate, bacterial content, bacterial growth stage, bacterial cell surface charge, and surface hyrophobocity.
Step 2 involves three phases:
Phase 1: Transport of the microbe to substrate surface and its attachment. Adherence factors includes fimbriae, pili, flagella, EPS (glycocalyx).
Phase 2: Microbial and substrate adherence phase to form bridge. These bridges which are formed in a combination of electrostatic attraction, covalent and hydrogen bonding, dipole interaction and hydrophobic interaction. Initial bond between the bacteria and substrate is weak slowly over a period they gain strength with polysaccharide adhesion or ligand formation.
Phase 3: specific microbial -substrate adherence phase which involves bonding of adhesin or ligand on the bacterial cell surface.
Step 3 involves bacterial growth and expansion. Monolayer of microorganisms attracts secondary colonizers to form microcolonies [15]. These microcolonies are similar to towers with lateral and vertical growth of microorganisms. Two types of microbial interaction are seen at cellular level during biofilm formation-co-adhesion and coaggregation [16]. Coadhesion is a process of recognition between a suspended cell and cell already attached to substratum. Coaggregation is a process where genetically distinct cells in suspension recognize each other and results in a clump formation. At the end of this stage biofilm is seen as corncob structure [17].
Step 4 involves the deattachment of biofilm microorganisms into their surroundings which are of two types -seeding disposal and clumping dispersal.
Seeding dispersal: it is a programmed detachment of Planktonic bacterial cells caused by local hydrolysis of the extracellular polysaccharide matrix, and conversion of a subpopulation of cells into motile planktonic cells. The detached cells are the ones which causes persistent infection [18].
Clumping Dispersal: A physical detachment pathway in which a fragment of a micro colony, simply detaches from the biofilm and is carried by the bulk until it lodges in a new location and initiates a
new sessile population. Deattachment can be of two types Erosion (continous deattachment of single cell) and Sloughing (rapid detachment of biofilm)
Electron microscopically Biofilms appears as tower or mushroom shaped microcolonies with interspersed channels that are separated from the external environment through which fluids move by convection [19].
Hypothesis For Root Canal Biofilm Formations
It is reasonable to assume that the preconditions for biofilm formation in the root canal vary depending on the cause of the pulpal breakdown. An ischemic injury by trauma, leading to pulpal necrosis, is likely to provide totally different prerequisites for the colonization phase than in a caries exposure of the pulp. In the latter case, the inflammatory lesion front may recede successively towards the apex, possibly in bursts, and provide the fluid vehicle by which invading planktonic organisms can multiply and start attaching to the root canal walls.
Implications Of Biofilm In Endodontics
Microorganisms present in the oral cavity serves as primary source of biofilm formation within the root canal. The anatomical complexities in the root canal system provide shelter to microorganisms [20]. Bacterial biofilm can be seen beyond the apex of the root as bacteria in biofilm survive unfavourable environmental and nutritional conditions [20], [21].
The necrotic pulp tissue becomes a favourable environment for microbial proliferation due to the presence of organic residue or nutrients, which act as substrate or culture medium. Gram-negative bacteria are more frequent than Gram-positive bacteria. Facultative or strict anaerobic microorganisms are more frequent than aerobic microorganisms, and the presence of bacilli and filaments is equivalent to that of cocci.
Endodontic biofilm can be of various categories:
1. Intracanal biofilm
2. Extra radicular biofilm
3. Periapical biofilm
4. Foreign body centered biofilm
Intracanal biofilm are microbial biofilm formed on the root canal dentine of infected tooth. First identification of biofilm was earlier reported by Nair 1987 under transmission electron microscopy [22]. Major bulk of the organisms existed as loose collections of cocci, rods, filaments and spirochetes apart from this bacterial condensation were seen as palisade structure similar to dental plaque seen on tooth surface [23]. The extracellular matrix material of bacterial origin was also found.
Extra radicular biofilm are root surface biofilms formed on root surface adjacent to the root apex of endodontically infected teeth [24]. In a study of cases resisting treatment (refractory endodontic cases) Tronstad et al examined root tips of surgical extracted teeth under SEM and found structureless smooth biofilm with multispecies bacteria and varying degree of extracellular matrix [25].
Lomcali et al [26] used SEM to examine root tips of asymptomatic apical periodontitis under which multilayered bacteria was seen embedded in a heavy extracellular matrix. Calculus like deposits was noticed at the root apex of extracted teeth after post treatment periapical periodontitis [27].
Periapical microbial biofilms are isolated biofilms in the periapical region of endodontically infected teeth. They can be seen even in the absence of root canal infections. Bacteria's present in such biofilm should have the capacity to overcome host defence mechanisms and result in periapical lesions [28]. Actinomyces species and P. Propionicum are associated with periapical lesions. Actinomyces species show the presence of yellow granules commonly referred as sulphur granules [29].
Microscopically these granules appear as ray fungus. The aggregation of Actinomyces cells are influenced by pH, ionic strength and cell concentration [30]. Aggregation facilitates biofilm formation.
Foreign body - centered biofilm is seen when bacteria adheres to an artificial biomaterial surface and forms biofilm structures [31]. It is also known as biomaterial centered infection. It is a major complication associated with prosthesis and also in an implant supported prosthesis. Biomaterial centered infection reveals opportunistic invasion by nosocomial organisms. In endodontics, biomaterial centered biofilm can be intraradicular or extraradicular depending upon the position of obturating material.
Role Of Enterococcus Faecalis In Biofilm:
Enterococcus faecalis the unique property of these organisms is biofilm formation and the physiochemical properties of organisms help them to modify according to the prevailing environmental and nutrient conditions. Biofilms formed by Enterococcus faecalis are able to resist destruction by enabling the bacteria to become 1000 times more resistant to phagocytoses, antibodies and antimicrobials than non biofilm producing bacteria [32].
Enterococcus faecalis forms biofilm in various stages which includes adherence of the organisms and formation of micro colonies followed by bacterial mediated dissolution of the mineral fraction from the dentin which results in release of calcium and phosphate ions leading to initial calcification. At later stages E. Faecalis biofilm shows carbonated -apatite structure as compared to natural dentine which contains carbonated flour apatite structure which are more resistant and difficult to eradicate [20]. Enterococcus faecalis co aggregates with F.nucleatum which results in further aggravate endodontic infection [33].
Apical Periodontitis Due To Biofilm
Apical periodontitis is a biofilm related chronic infectious disease that occurs very frequently.
Apical periodontitis is an inflammatory process in the periradicular tissues caused by microorganisms in the necrotic root canal. Accordingly, to achieve healing of apical periodontitis, the main goal of the treatment must be elimination of the infection and prevention of re-infection.
Once endodontic therapy has been initiated, several factors may potentially contribute to breakdown of the periapical tissues, resulting in persistence of the disease process. These factors include complications such as perforations, instrument fractures, and extrusion of materials used during the treatment in the periapical area.
In addition, development of a radicular cyst or cholesterol crystals may contribute to persistence of disease after endodontic treatment
The etiology of apical periodontitis in a root-filled tooth (post-treatment disease) is generally the same as in primary apical periodontitis: microbial infection of the root canal. However, the root-filled tooth and the root canal(s) have already undergone a variety of treatment procedures, including use of mechanical instruments such as burs, and files, local disinfecting agents such as irrigants, and inter-appointment dressings and root filling. Consequently, secondary factors are often highlighted when persistence of disease is analyzed. Nevertheless, as indicated earlier, without the presence of a microbial infection, mechanical complications related to technical procedures and use of materials do not cause more than temporary problems such as short-lasting (aseptic) inflammatory reaction due to physical or chemical trauma and the occasional occurrence of pain [39].
Anti-microbial Agents And Biofilms
Central to the theme of biofilm control is the use of surfactants, anti-microbial agents and preservatives.
Anti-microbial agents have often been developed and optimized for their activity against fast growing, dispersed populations containing a single micro-organism. However, microbial communities grown in biofilms are remarkably difficult to eradicate with anti-microbial agents and microorganisms in mature biofilms can be notoriously resistant for reasons that have yet to be adequately explained. There are reports showing that microorganisms grown in biofilms could be two- to 1000-fold more resistant than the corresponding planktonic form [34], [35]. With respect to oral bacteria, the biofilm inhibitory concentrations for chlorhexidine and amine fluoride are 300 and 75 times greater, respectively, when Streptococcus sobrinus is grown as a biofilm compared with the minimum bactericidal concentration for planktonic cells [36]. Biofilms of oral bacteria have also been found to be more resistant to amoxycillin, doxycycline and metronidazole [37].
Removal Of Biofilm:
The structural dense organization of the biofilm within the polymeric matrix restricts the penetration of any agent into them. Biofilm are found to be resistant to amoxicillin, doxycycline and metronidazole [36].
Sodium hypochlorite is an effective irrigant to destroy all forms of Enterococcus faecalis including its biofilm form [37]. Chlorhexidine 2% gel or liquid form is effective to eliminate Enterococcus faecalis from the superficial layers of dentinal tubules up to 100micrometer.50
The new techniques include use of ultrasonic irrigation, ozone, plasma dental probe, photoactivated disinfection with low-energy laser for biofilm removal. 1-minute use of ultrasonically activated irrigation, followed by root canal cleaning and shaping has been shown to improve canal and isthmus cleanliness in terms of necrotic debris/biofilm removal.
High concentrated gaseous and aqueous ozone is strain, dose and time dependently effective against the tested microorganisms in suspension and biofilm test model. However, NaOCl was the only method that eliminated biofilm.
Plasma dental probe is effective for tooth disinfection. Scanning electron microscopy shows complete destruction of endodontic biofilms for a depth of 1 mm inside a root canal after plasma treatment for 5 min.
Plasma emission spectroscopy identifies atomic oxygen as one of the likely active agents for the bactericidal effect.
The Er:YAG laser have produced excellent results due to its capacity for ablating hard tissue with very less thermal effects. They are considered to be effective tool for the removal of apical biofilm.
Photodynamic therapy/ Light Activated Therapy is the latest method used to destruct endodontic biofilm. It involves the killing of microorganisms when a photo sensitizer selectively accumulated in the target is activated by a visible light of appropriate wavelength. PAD is a unique combination of a photosensitizer solution and low-power laser light. The photosensitizer, which is mostly colored, adheres to or gets absorbed by microbial cells. The low-power laser will destruct the target area and inactivate the microbial invaders.
Usually sodium hypochlorite, antibiotics and other methods against microbial threats need a lot of time to inactivate the microbes. PAD needs a maximum of 150 seconds. PAD is effective against Enterococcus faecalis, Streptococcus intermedius, Fusobacterium nucleotum, Peptostreptococcus micros, Prevotella intermedia)
Root Canal Disinfection
The application of PDT in clinical practice is as follows:
The photoactive drug will be applied in the root canal system after instrumentation is complete for a short time (up to five minutes) and will strongly bind to the negatively charged matrix and to bacteria. Then a fiber optic will be used to deliver red light from a diode laser to irradiate microbial biofilms on the root canal surface as well as in the dentinal tubules. The entire root canal system will be exposed to light simultaneously for five minutes.
Conclusions
The surface-associated growth of microorganisms is the cause of most endodontic infection.
The application of the biofilm concept to endodontic microbiology will play a crucial role in helping us to understand, not only the pathogenic potential of the root canal microbiota, but also the basis for new approaches for disinfection. Microorganisms adaptation under different disease conditions as well as how biofilms are organized in root canals are important issues to be addressed on the road to obtain a clear understanding of how the root canal bacteria resist endodontic treatment measures.
References
1. Bowden GH, Hamilton IR. Survival of oral bacteria. Crit Rev Oral Biol Med 1998: 9 54-84.
2. Tronstad L, Barnett F, Cervone F. Periapical bacterial plaque in teeth refractory to endodontic treatment. Endod Dent Traumatol 1990: 6 73-77.
3. Leonardo MR, Rossi MA, Silva LAB, Ito IY, Bonifa´cio C. EM evaluation of bacterial biofilm and microorganisms on the apical external root surface of human teeth. J Endod 2002: 28 815-818.
4. Siqueira JF, Lopes HP. Bacteria on the apical root surfaces of untreated teeth with periradicular lesions: a scanning electron microscopic study. Int Endod J 2001: 34 216-220.
5. Noiri Y, Ehara A, Kawahara T, Takemura N, Ebisu S. Participation of bacterial biofilms in refractory and chronic periapical periodontitis. J Endod 2002: 28 679-683.
6. Lomcali G, Sen BH, Cankaya H. Scanning electron microscopic observations of apical root surfaces of teeth with apical periodontitis. Endod Dent Traumatol 1996: 12 70-76.
7. Ferreira FBA, Ferreira AL, Gomes BPF, Souza-Filho FJ. Resolution of persistent periapical infection by endo-dontic surgery. Int Endod J 2004: 37 61-69.
8. Nair PNR. Light and electron microscopic studies on root canal flora and periapical lesions. J Endod 1987: 13 29-39.
9. Molven O, Olsen I, Kerekes K. Scanning electron microscopy of bacteria in the apical part of root canals in permanent teeth with periapical lesions. Endod Dent Traumatol 1991: 7 226-229.
10. Barrieshi KM, Walton RE, Johnson WT, Drake DR. Coronal leakage of mixed anaerobic bacteria after obturation and post space preparation. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997: 84 310-314.
11. Distel JW, Hatton JF, Gillespie MJ. Biofilm formations in medicated root canals. J Endod 2002: 28 689-693.
12. Hubble TS, Hatton JF, Nallapareddy SR, Murray BE, Gillespie MJ. Influence of Enterococcus faecalis proteases and the collagen-binding protein, Ace, on adhesion to dentin. Oral Microbiol Immunol 2003: 18 121-126.
13. Beighton D, Smith K, Hayday H. The growth of bacteria and production of exoglycosidic enzymes in the dental plaque of macaque monkeys. Arch Oral Biol 1986; 31:829-835.
14. Kolenbrander PE et al. Communication among oral bacteria. Microbial Mol Biol Rev 2002; 66:486-505.
15. Cowen M, Taylor KG, Doyle RJ. Energetic of the initial phase of adhesion of Streptococcus sanguis to hydroxyappatite . J Bacteriol 1987; 169:2995-3000.
16. Busscher H, Van der Mei HC. Physico-chemical interactions in intial microbial adhesion and relevance for biofilm formation. Adv Dent Res 1997; 11(1): 24-32.
17. Kolenbrander P et al. Intergeneric coaggregation of oral Treponema species with Fusobacterium species and intrageneric coaggregation among Fusobacterium species. Infect Immun 1995;63:4584-8.
18. Debeer D, Stoodley P, Roe F, Lewandowski Z. Effects of biofilm structures on oxygen distribution and mass transport. Biotechnol Bioeng 1994; 11(43): 1131-8.
19. Lawrence JR,Korber DR, Hoyle BD, Costerton DE. Optical sectioning of microbial biofilms. J Bacteriol 1991; 173: 6558-67.
20. Mory F, Fougnot S, Rabaud C et al . In vitro activities of cefotaxime, vancomycin, quinupristin/dalfopristin,linezolid and other antibiotic alone and in combination against Propiobacterium acnes isolates from central nervous system infections. J Antimicrob Chemother 2005;55(2): 265-8.
21. Figdor D. Apical periodontitis: a very prevalent problem. Oral Surg Oral Med Oral Pathol 2002;6(94):651-2.
22. Nair PNR . Light and electron microscopic studies on root canal flora and periapical lesions. J Endod 1987;13: 29-39.
23. Listgarten M . Formation of dental plaque and other biofilms In: Newman HN, Wilson M eds. Dental Plaque Revisited. Oral Biofilms in Health and Disease. Cardiff: Bioline, 1999: 187-210.
24. Frank SA, Barbour AG. Within -host dynamics of antigenic variation. Infect Genet Evol 2006;6(2): 141-6
25. Tronstad L, Barnett F , Cervone F . Periapical bacterial plaque in teeth refractory to endodontic treatment. Endod Dent Traumatol 1990 ; 6:73-77.
26. Lomacali G, Sen BH, Cankaya H . scanning electron microscopic observations of apical root surfaces of teeth with apical perriodontitis. Endod DENT Traumatol 1996;12:70-76.
27. Ricicci D, Martorano M , Bate AL , Pascon EA . Calculus-like deposit on the apical external root surface of teeth with post treatment apical periodontitis: report of two cases. Int Endod J 2005;38:262-71.
28. Medvedev AE,Sabroe I, Hasday JD, Vogel SN. Tolerance to microbial TLR ligands: molecular mechanisms and relevance to disease. J Endotoxin Res 2006;12(3):133-50.
29. Jontell M, Gunraj MN, Bergenholtz G. Immunocompetent cells in the normal dental pulp. J Dent Res 1987;66(6):1149-53.
30. Miller C et al Factors affecting the aggregation of Actinomyces naeslundii during growth and in washed cell suspensions. Infect Immun 1979;21(3): 1003-9.
31. Wilson M. Susceptibility of oral bacterial biofilm to antimicrobial agents. J Med Microbiol 1996;44(2):79-87.
32. Distel JW, Hatton JF, Gillespie MJ. Biofilm formation in medicated root canals. J Endod 2002; 28:689-93.
33. Siren EK, Haapasalo MP,Ranta K et al. Microbiological findings and clinical treatment procedures in endodontic cases selected for microbiological investigation. Int Endod J 1997;30(2):91-5.
34. Gilbert P, Das J, Foley I. Biofilm susceptibility to antimicrobials. Adv Dent Res 1997: 11 160-167.
35. Johnson SA, Goddard PA, Iliffe C, Timmins B, Rickard AH, Robson G, Handley PS. Comparative susceptibility of resident and transient hand bacteria to para-chloro-meta- xylenol and triclosan. J Appl Microbiol 2002: 93 336-44.
36. Shani S, Friedman M, Steinberg D. The anticariogenic effect of amine fluorides on Streptococcus sobrinus and glucosyltransferase in biofilms. Caries Res 2000: 34 260-267.
37. Larsen T. Susceptibility of Porphyromonas gingivalis in biofilms to amoxicillin, doxycycline and metronidazole. Oral Microbiol Immunol 2002: 17 267-271.
38. Spratt DA, Pratten J, Wilson M, Gulabivala K. An in vitro evaluation of the antimicrobial efficacy of irrigants on biofilms of root canal isolates. Int Endod J 2001: 34 :300-307.
39. Persistent, recurrent, and acquired infection of the root canal system post-treatment Markus Haapasalo, Trude Udnæs, & Unni Endal Endodontic Topics 2003, 6 29-56 |