Introduction
Probiotic are living microbial organisms that can benefit our health. The term "probiotic" is derived from the Latin preposition pro ("for") and the Greek adjective (biotic), the latter deriving from the noun (bios, "life"). [1], [2], [3] Probiotic may modify the microbial balance of the host by reducing the overgrowth of the pathogens. They are now becoming more widely used, usually in form of foods and food supplements.
In past few years probiotics have been investigated in oral health prospective. Oral infections constitute some of the most common and costly forms of infections in humans. The concept of microbial ecological change as a mechanism for preventing dental disease is an important concept while altered microbial ecology may lead to dental disease. New methods such as probiotic approaches (i.e. whole bacteria replacement therapy) to replace pathogenic members of the microbiota by using harmless bacteria are now being widely used to combat infections. Limited research is available showing that some probiotic cultures may help dental improvement. This review article mainly focuses on the current opinion of possible oral benefits of probiotics.[1]
Historical Background
In 1907 the Ukrainian-born biologist and Nobel laureate Elie Metchnikoff realized that consumption of Bulgarian yoghurt (which contains lactic acid bacteria) was good for health who suggested that "The dependence of the intestinal microbes on the food makes it possible to adopt measures to modify the flora in our bodies and to replace the harmful microbes by useful microbes".[1]
At that time Henry Tissier (1906), a French paediatrician, observed that children with diarrhea had in their stools a low number of bacteria characterized by a peculiar, Y shaped morphology. These "bifid" bacteria were, on the contrary, abundant in healthy children. He suggested that these bacteria could be administered to patients with diarrhea to help restore a healthy gut flora.
Metchnikoff worked at the Pasteur Institute in Paris and had discovered Lactobacillus bulgaricus, a strain he later introduced into commercial production of sour-milk products in France and throughout Europe. The concept of probiotics was thus born and a new field of microbiology and was opened.[2]
It was first used by Lilly and Stillwell[4] in 1965 to describe "substances secreted by one micro-organism which stimulates the growth of another" and thus was contrasted with the term antibiotic. Since then various definitions for probiotics have been proposed.
Definitions of Probiotics:-
According to The Food Agricultural Organization (FAO) and World Health Organization (WHO) report (2001), probiotics are "Live micro-organisms which, when administered in adequate amounts, confer a health benefit on the host".
International Life Science Institute (ILSI) Europe suggests a definition according to which a probiotic is "a live microbial food ingredient that, when ingested in sufficient quantities, exerts health benefits on the consumer". Both definitions have in common the idea that probiotic micro-organisms are living and exert proven health effects.[5]
Schrezemeir J & Michel de Vrese[6] described "A preparation of, or a product containing, viable, defined microorganisms in sufficient numbers, which alter the microflora (by implantation or colonization) in a compartment of the host and as such exert beneficial health effects in this host".
Marteau et al, in 2002 defined them as "microbial preparations or components of microbial cells that have a beneficial effect on health and well-being".[7]
What are Probiotics and Synbiotics?
The term Prebiotic was introduced by Gibson and Roberfroid.[8] Prebiotic is a non-digestible food ingredient that confers benefits on the host by selectively stimulating the growth and/or activity of one bacterium or a group of bacteria in the colon, and thus improves the host health. Prebiotics are dietary carbohydrates that escape digestion in the upper gastrointestinal tract, alter the bacterial composition of the gut, by changing the type of the substrate provided to the existing microbial population in the gut e.g. fructo-oligosaccharides, gluco-oligosaccharides and insulin.
The term Synbiotic is used when a product contains both probiotics and prebiotics. Because the word alludes to synergism, this term should be reserved for products in which the prebiotic compound selectively favors the probiotic compound.[6]
Vehicles of administration [9], [10]
Probiotics are provided in products in one of four basic ways:
As a culture concentrate added to a beverage or food (such as fruit juice),
Inoculated into Prebiotic fibers,
Inoculated into a milk-based food (dairy products such as milk, milk drink, yoghurt, yoghurt drink, cheese, kefir, bio-drink) and
As concentrated and dried cells packaged as dietary supplements (non-dairy products such as powder, capsule, gelatin tablets). The different probiotics in oral health are tabulated (Table-I).
 | Table 1: Name of the microorganisms used as probiotics9
 |
Mechanism of Action
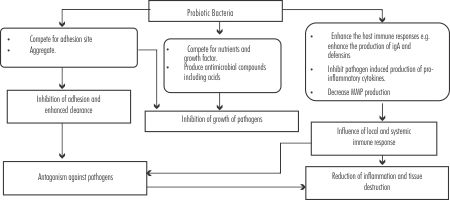
The mechanisms by which probiotics exert their effects are largely unknown, but may involve modifying gut pH (normalization of intestinal microbiota), antagonizing pathogens through production of antimicrobial compounds (organic acids, hydrogen peroxide, and bateriocins), competing for pathogen binding and receptor sites as well as for available nutrients and growth factors, stimulating immune modulatory cells, and producing lactase. Probiotic bacteria have been shown to influence the immune system through several molecular mechanisms.[11],[12] The mechanisms of probiotic action in the oral cavity could be analogous to those described for the intestine. In oral cavity, probiotics tend to create a biofilm, acting as a protective lining for oral tissues against oral diseases. Such a biofilm keeps bacterial pathogens off oral tissues by filling a space which could have served as a niche for pathogens in future; and competing with cariogenic bacteria and periodontal pathogens growth.[1] [Figure-1], summarizes the possible mechanism by which Probiotic Bacteria might affect oral health.[3], [12], [13], [14]
Probiotics in General Health
1. Reduction of the concentration of cancer-promoting enzymes and/or putrefactive (bacterial) metabolites in the gut.
2. Prevention and alleviation of unspecific and irregular complaints of the gastrointestinal tracts in healthy people.
3. Prevention of respiratory tract infections (common cold, influenza) and other infectious diseases as well as treatment of urogenital infections.
4. Prevention and/or reduction of duration and complaints of rotavirus-induced or antibiotic-associated diarrhoea as well as alleviation of complaints due to lactose intolerance.
5. Prevention or alleviation of allergies and atopic diseases in infants.
6. Normalization of passing stool and stool consistency in subjects suffering from constipation or an irritable colon.
7. Beneficial effects on microbial aberrancies, inflammation and other complaints in connection with: inflammatory diseases of the gastrointestinal tract, helicobacter pylori-infection or bacterial overgrowth.[13]
Probiotics in Oral Health
As the bacterial resistance to antibiotics is emerging wide spreadly, the concept of probiotic therapy has been considered for application in oral health. Dental caries, periodontal disease, halitosis, and oral candidosis are among the oral disorders that have been targeted. An essential condition for a microorganism to represent a probiotic of interest for oral health is its capacity to adhere to and colonize various surfaces of the oral cavity.[12] Lactobacilli constitutes about 1% of the cultivable oral microflora in humans. Lactobacilli are extremely aciduric and can withstand a pH as low as 3.5, which is a prerequisite to survive the low-pH transition into the intestines. Bifidobacteria are the predominant anaerobic bacteria naturally occurring within the small intestinal lumen and play a critical role in maintaining the equilibrium among normal.[14] The survival of various probiotics used by the dairy industry (specifically, species of both Lactobacillus and Bifidobacterium) in saliva and their adherence to oral surfaces was assessed by Haukioja et al.[15] They found that all of the tested strains survived well in saliva, but they varied widely in their capacity to adhere to the surface of teeth and oral mucosa. More specifically, species in the genus Lactobacillus had an adherence capacity superior to that of the Bifidobacteriumn species.[15]
Probiotics and Dental Caries
To have a beneficial effect in limiting or preventing dental caries, a probiotic must be able to adhere to dental surfaces and integrate into the bacterial communities making up the dental biofilm. It must also compete with and antagonize the cariogenic bacteria and thus prevent their proliferation.[12]
Probiotics can reduce the risk fora high Streptococcus mutans (S. mutans) level occurrence.[16] In a recent study by Çaglar et al.,[17] the effect of xylitol and probiotic chewing gums on salivary Streptococci mutans and Lactobacilli was evaluated. A reduced S. mutans level was observed in subjects using probiotics or xylitol enriched chewing gum. However, no synergic effect was seen when combining both agents.
Nikawa et al.[18] reported that consumption of yoghurt containing Lactobacillus reuteri (L. reuteri) over a period of 2 weeks reduced the concentration of S. mutans in the saliva by up to 80%. In a study by Nase et al.[19] they found that children consuming milk containing probiotic, particularly those 3-4 years of age, had significantly fewer dental caries and lower salivary counts of S. mutans than controls. These promising results suggest a potentially beneficial application of probiotics for the prevention of dental caries. It has been suggested that the operative approach in caries treatment might be challenged by probiotic implementation with subsequent less invasive intervention in clinical dentistry. More studies are definitely needed before this goal could be achieved.[20]
Probiotics and Periodontal Disease
The first studies of the use of probiotics for enhancing oral health were for the treatment of periodontal inflammation.[21] The main pathogenic organisms associated with periodontitis include Provitellagingivalis, Treponemadenticola, Tannerella forsythia etc. Various studies have reported the capacity of lactobacilli to inhibit the growth of periodontal pathogens, including P. gingivalis, Prevotellaintermedia and A. Actinomycetemcomitans. Together, these observations suggest that lactobacilli residing in the oral cavity could play a role in the oral ecological balance.[22] Patients with various periodontal diseases, gingivitis, periodontitis, and pregnancy gingivitis, were locally treated with a culture supernatant of a L. acidophilus strain. Significant recovery was reported for almost every patient. There has been significant interest in using probiotics in treatment of periodontal disease recently, too. The probiotic strains used in these studies include L. reuteri strains, L. brevis (CD2), L. caseishirota, L. salivarius WB21, and Bacillus subtilis. L. reuteri and L. brevis have improved gingival health, as measured by decreased gum bleeding.[22], [23] The use of probiotic chewing gum containing L. reuteri ATCC 55730 and ATCC PTA 5289 also decreased levels of pro-inflammatory cytokines in GCF, [24] and the use of L. brevis decreased MMP (collagenase) activity and other inflammatory markers in saliva.[23] B. subtilis seemed to reduce the number of periodontal pathogens. [25] Use of tablets containing L. salivarius WB21 has been shown to decrease gingival pocket depth, particularly in high-risk groups such as smokers, and also affect the number of periodontal pathogens in plaque. [26] Again, although encouraging results have been observed, most studies have been fairly short. Furthermore, in some studies the observed differences were quite small, though statistically significant.
Probiotics and halitosis (Oral malador)
Oral halitosis (malador) refers to bad breath originating from the oral cavity. It regularly affects about one in four adults and frequently is caused by anaerobic bacteria that degrade salivary and food proteins to generate amino acids, producing volatile sulfur compounds (VSCs).[27] Halitosis is considered to be an aesthetic problem, with multiple local and systemic etiological factors. The main local etiologies include periodontitis, poor oral hygiene, deep dental caries, tongue coating, and faulty restorations.
"Physiologic" is a term used to describe halitosis as the result of imbalance of the microbiota in the oral cavity without any organic lesion, in contrary to "pathologic" halitosis where patients usually presented with organic lesion most commonly periodontitis.
A recent study has shown that patients with genuine physiologic or pathologic halitosis benefited significantly from two-week therapy with tablets containing L. salivariusWB21 in addition to a significant reduction in the level of the volatile compounds and gingival bleeding on probing from periodontal pockets. [28] Lactobacillus salivarius TI2711 bacteria were also able to reduce the count of the oral black pigmented bacteroides, the bacteria that is strongly associated with production of the volatile sulphur compounds responsible for halitosis.[29] A study by Kang et al. (30) reported that gargling with a solution containing various strains of Weissella Cibaria (W. Cibaria) has ability to decrease the production of volatile sulphur compounds (hydrogen sulphide and methanethiol) by Fusobacterium nucleatum (F. Nucleatum). Various probiotic products are marketed for both mouth and gut associated halitosis, although their efficacy demands more clinical studies.[30]
Probiotics and Oral Candidosis
Candida species constitute part of the commensal oral flora in about 50% of healthy subjects, but able to cause a clinically apparent lesion if the immune defenses were breached either on the local or systemic level.[31] One study has shown that the subjects who consumed cheese containing the probiotic L. rhammnosus GG and Propionibacterium freudenreichiisp[32] exhibited reduction in the prevalence of oral Candid [33] which subsequently may confer protective effect against oral candidosis. A concomitant feature of the probiotic activity observed in this study was the diminished risk of hypo salivation and the feeling of dry mouth of the subjects.[32] However, others investigated the effect of various lactobacilli and could not find an effect on oral Candida.[34] This may be partly explained by the finding of the ex vivo experiment which demonstrated a profound but variable abilities of commercially available strain of lactobacilli probiotics to inhibit the growth of C. albicans possibly due to the low pH milieu produced by the lactobacilli.[35] Relevant to this is the laboratory study which demonstrated that the Candida-infected mice which were fed with L. acidophilus exhibited accelerated clearance of C. albicans from the mouth.[36]
Safety Issues
Different strains of same species may possess different characteristics, necessitating rigorous strain selection before being labeled as probiotic. Some probiotic strains have been in use for many years and have excellent safety records.[37] Probiotics are live micro-organisms and hence, it is possible that they may result in infection in the host. Although probiotic therapy is generally considered safe, the concept of willingly ingesting live bacteria remains somewhat counter intuitive. Systemic infection has rarely been reported with Bifidobacterium , although many cases of sepsis secondary to Lactobacillus rhamnosus GG or Lactobacillus casei have been reported [38], [39] The risk and morbidity of sepsis due to probiotic bacteria should be weighed against the potential for sepsis due to more pathological bacteria and the morbidity of the diseases for which probiotic bacteria are being used as therapeutic agents. The reports of sepsis are mainly seen in immune-compromised or infants.[38], [39]
Maybe because long-term colonization of oral cavity by probiotic bacteria is unlikely, albeit possible, potential adverse effects of probiotic bacteria in the oral cavity have not been a subject of much intensive research; however, probiotic products are used widely; therefore, when dental health is considered, the acidogenicity of lactobacilli and bifidobacteria cannot be overlooked. For example, one L. salivarius strain is able to induce caries in an animal model, [40] and another is able to make a biofilm model more cariogenic.[42]
Future Strategies
Genetically modified microbes bring a new dimension to the concept of probiotics. Their main thrush is on reducing the harmful properties of pathogenic strains naturally colonizing the oral cavity. The modified strain could then be used to replace the original pathogen. One ambitious and promising example is the generation of an S. mutans strain with a complete deletion of the open reading frame of lactate hydrogenase and thus significantly reduced cariogenicity.[42] Another option could be to enhance the properties of a potentially beneficial strain. One example is the construction of an L. paracasei strain with a functional scFV (single-chain variable fragment) antibody binding to the surface of Porphyromonasgingivalis.[43] Therefore; the new probiotic products targeted for oral health purposes do not necessarily comprise the same species as products now in market.
Potential future uses of probiotics include inflammatory disease control, the treatment, and prevention of allergies, cancer prevention, immune stimulation, and a reduction in respiratory disease. Such effects could justify the addition of not one but potentially several probiotics to commonly consumed foods, which could achieve population-wide health benefits. In field of oral immunology, probiotics are being used as passive local immunization vehicles against dental caries (C3). Bacteriophages, viruses that kill bacteria, have been detected in oral pathogens, such as Actinobacillus actinomycetemcomitans, and they may play a role in the pathogenicity. Subsequently, future studies should be conducted to investigate if phage therapy might be applied for oral and dental diseases in the same way as has been attempted for systemic infections. The selection of the best probiotic for oral health is also an issue that calls for further study.
Conclusion
The interest in oral probiotics has been growing since the last few decades. Probiotics are, nevertheless, a new and interesting field of research in oral microbiology and oral medicine. Most of the studies have been conducted with probiotic strains originally suggested for gut health. A literature reviews shows that probiotics use in associated to an improvement in oral health, which is mainly due to significantly reduced levels of cariogenic as well as periodontal pathogens.
The concept casts new light on the connections between diet and health, including oral health. They are probably going to play an important role in combating problems arising from overuse of antibiotics and antimicrobial resistance.[10] Milk, milk drinks, or yoghurt containing one or more probiotic strains could be a treatment option in the long-term prevention of childhood caries.[14] Some of these technologies may be parenterally administered to treat life-threatening infections and emerging drug-resistant organisms.[20] The influx of studies expected in the coming years, will most likely clarify some of these issues.
References:
1. Report of a joint FAO/WHO expert consultation and evaluation of health and nutritional properties of probiotics in food including powder milk with live lactic acid bacteria Cordoba, Argentina. 1 - 4 October 2001
2. Meurman JH. Probiotics: do they have a role in oral medicine and dentistry? Eur J Oral Sci. 2005; 113:188-96.
3. Hamilton-Miller JMT, Gibson GR, Bruck W. "Some insights into the derivation and early uses of the word 'probiotic". Br J Nutr. 2003; (90):845.
4. Lilly DM, Stillwell RH. Probiotics. Growth promoting factors produced by microorganisms. Science. 1965; 147:747-748.
5. Schrezenmeir J, de Vrese, M. Probiotics, prebiotics, and synbiotics. Adv Biochem Eng Biotechnol. 2008;111:1-66.
6. Schrezenmeir J, de Vrese M. Probiotics, prebiotics, and synbiotics-approaching a definition. Am J Clin Nutr. 2001; 73(suppl):361S-364S.
7. Limdi JK, O Neill C, McLaughlin J. Do probiotics have a therapeutic role in gastroenterology? World Journal of Gastroenterology. 2006; 12(34):5447-57.
8. Gibson GR, Roberfroid MB. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. Journal of Nutrition. 1995; 125:1401-1412.
9. Alvarez-Olmos MI, Oberhelman RA. Probiotic agents and infectious diseases: A modern perspective on a traditional therapy. Clin Infect Dis. 2001;32:1567- 76.
10. E Caglar, B Kargul, Tanboga. Bacteriotherapy and probiotics role on oral health. Oral Diseases. 2005; 11:131-137.
11. S Parvez, KA Malik, S Ah Kang, HY Kim. Probiotics and their fermented food products are beneficial for health Journal compilation 2006 The Society for Applied Microbiology. Journal of Applied Microbiology. 2006; 100:1171-1185.
12. Bonifait L, Chandad F, Grenier D. Probiotics for Oral Health: Myth or Reality?. J Can Dent Assoc. 2009; 75: 585-90.
13. de Vrese. M, Schrezenmeir.J. Probiotics, prebiotics and synbiotics. Food Biotechnology. 2008:1-66.
14. Twetman S, Stecksen-Blicks C. Probiotics and oral health effects in children. Int J Paediatr Dent. 2008; 18: 3-10.
15. Haukioja A, Yli-Knuuttila H, Loimaranta V, Kari K, Ouwehand AC, Meurman JH, et al. Oral adhesion and survival of probiotic and other lactobacilli and bifidobacteria in vitro. Oral Microbiol Immunol. 2006; 21(5): 326-32.
16. Flichy-Fernandez AJ, Alegre-Domingo T, Penarrocha-Oltra D, Penarrocha-Diago M. Probiotic treatment in the oral cavity: an update. Med Oral Patol Oral Cir Bucal. 2010; 15(5): e677-80.
17. Çaglar E, Kavaloglu SC, Kuscu OO, Sandalli N, Holgerson PL, Twetman S. Effects of chewing gums containing xylitol or probiotic bacteria on salivary mutans streptococci and lactobacilli. Clin Oral Investig. 2007; 11: 425-9.
18. Nikawa H, Makihira S, Fukushima H, Nishimura H, Ozaki K, Ishida K, et al. Lactobacillus reuteri in bovine milk fermented decreases the oral carriage of mutans streptococci. Int J Food Microbiol. 2004; 95: 219-23.
19. Nase L, Hatakka K, Savilahti E, Saxelin M, Pönkä A, Poussa T, et al. Effect of long-term consumption of a probiotic bacterium, Lactobacillus rhamnosus GG, in milk on dental caries and caries risk in children. Caries Res. 2001; 35:412-20.
20. Anderson M, Shi W. A probiotic approach to caries management.Pediatric dentistry. 2006; 28(2):151-3.
21. Mager DL, Ximenez-Fyvie LA, Haffajee AD, Socransky SS. Distribution of selected bacterial species on intraoral surfaces. J ClinPeriodontol. 2003; 30:644-54.
22. KõllKlais P, Mändar R, Leibur E, Marcotte H, Hammarström L, Mikelsaar M. Oral lactobacilli in chronic periodontitis and periodontal health: species composition and antimicrobial activity. Oral microbiology and immunology. 2005; 20(6):354-61.
23. Della Riccia DN, Bizzini F, Perilli MG, Polimeni A, Trinchieri V, Amicosante G, et al. Anti-inflammatory effects of Lactobacillus brevis (CD2) on periodontal disease. Oral Dis. 2007; 13:376-85.
24. Twetman S, Derawi B, Keller M, Ekstrand K, Yucel-Lindberg T, Stecksen-Blicks C. Short-term effect of chewing gums containing probiotic Lactobacillus reuteri on the levels of inflammatory mediators in gingival crevicular fluid. Acta Odontol Scand. 2009; 67:19-24.
25. Tsubura S, Mizunuma H, Ishikawa S, Oyake I, Okabayashi M, Katoh K, et al. The effect of Bacillus subtilis mouth rinsing in patients with periodontitis. Eur J ClinMicrobiol Infect Dis. 2009; 28:1353-56.
26. Mayanagi G, Kimura M, Nakaya S, Hirata H, Sakamoto M, Benno Y, et al. Probiotic effects of orally administered Lactobacillus salivarius WB21- containing tablets on periodontopathic bacteria: a double-blinded, placebo controlled, randomized clinical trial. J Clin Periodontol 2009;36:506-13.
27. Haraszthy VI, Zambon JJ, Sreenivasan PK, Zambon MM, Gerber D, Rego R, et al. Identification of oral bacterial species associated with halitosis. J Am Dent Assoc. 2007; 138: 1113-20.
28. Iwamoto T, Suzuki N, Tanabe K, Takeshita T, Hirofuji T. Effects of probiotic Lactobacillus salivarius WB21 on halitosis and oral health: an open-label pilot trial. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 110:201-8.
29. Matsuoka T, Sugano N, Tanigawa S, Takane M, Yoshimura N, Ito K, et al. Effect of oral Lactobacillus salivarius TI 2711 (LS1) administration on periodontopathic bacteria in subgingival plaque. J Jpn Soc Periodontol. 2006; 48:315-24.
30. Kang MS, Kim BG, Chung J, Lee HC, Oh JS. Inhibitory effect of Weissellacibaria isolates on the production of volatile sulphur compounds. J Clin Periodontol. 2006; 33:226-32.
31. Darwazeh AM, Al-Dosari A, Al-Bagieh NH. Oral Candida and Aspergillus flora in a group of Saudi healthy dentate subjects. Int Dent J. 2002; 52: 273-7.
32. Maukonen J, Mättö J, Suihko ML, Saarela M. Intra-individual diversity and similarity of salivary and faecalmicrobiota. Journal of medical microbiology. 2008; 57(12):1560-8.
33. Hatakka K, Ahola AJ, Yli-Knuuttila H, Richardson M, Poussa T, Meurman JH, et al. Probiotics reduce the prevalence of oral Candida in the elderly--a randomized controlled trial. J Dent Res. 2007; 86:125-30.
34. Koll P, Mandar R, Marcotte H, Leibur E, Mikelsaar M, Hammarström L. Characterization of oral lactobacilli as potential probiotics for oral health. Oral Microbiol Immunol. 2008; 23:139-47.
35. Hasslof P, Hedberg M, Twetman S, Stecksen-Blicks C. Growth inhibition of oral mutans streptococci and Candida by commercial probiotic lactobacilli-an in vitro study. BMC Oral health. 2010; 2:10-18.
36. Elahi S, Pang G, Ashman R, Clancy R. Enhanced clearance of Candida albicans from the oral cavities of mice following oral administration of Lactobacillus acidophilus. Clin Exp Immunol. 2005; 141:29-36.
37. Husni RN, Gordon SM, Washington JA, Longworth DL. Lactobacillus bacteremia and endocarditis: review of 45 cases. Clin Infect Dis. 1997; 25: 1048-55.
38. Simhon A, Douglas JR, Drasar BS, Soothill JF. Effect of feeding on infants' faecal flora. Arch Dis Child. 1982; 57:54-58.
39. Adlerberth I, Carlsson B, de Man P, Jalil F, Khan SR, Larsson P, et al. Intestinal colonization with Enterobacteriaceae in Pakistani and Swedish hospital-delivered infants. Acta Paediatr Scand. 1991; 80:602-10.
40. Matsumoto M, Tsuji M, Sasaki H, Fujita K, Nomura R, Nakano K, et al. Cariogenicity of the probiotic bacterium Lactobacillus salivarius in rats. Caries Res. 2005; 39: 479-83.
41. Pham LC, van Spanning RJ, Roling WF, Prosperi AC, Terefework Z, Ten Cate JM, et al. Effects of probiotic Lactobacillus salivarius W24 on the compositional stability of oral microbial communities. Arch Oral Biol 2009;54:132-37.
42. Hillman JD, Mo J, McDonell E, Cvitkovitch D, Hillman CH. Modification of an effector strain for replacement therapy of dental caries to enable clinical safety trials. J Appl Microbiol. 2007; 102:1209-19.
43. Marcotte H, Koll-Klais P, Hultberg A, Zhao Y, Gmur R, Mandar R, et al. expression of single-chain antibody against RgpA protease of Porphyromonasgingivalis in Lactobacillus. J Appl Microbiol 2006; 100:256-63. |