Introduction
Edward H. Angle described a Class III malocclusion as one in which the lower first molar is mesially positioned relative to the upper first molar[1]. This relationship may result from a normal maxilla and mandibular skeletal protrusion or a maxillary retrusion and a normal mandible or a combination of maxillary retrusion and mandibular protrusion. A Class III dental relationship could also exist in a patient concave facial profile, and the lower lip often is protruded relative to the upper lip. Sometimes a Class III relationship is caused by a forward shift of the mandible to avoid incisal interferences. This is a pseudo Class III malocclusion[2]. The influence of environmental factors and oral function on the etiologic factors of a Class III malocclusion is not understood completely[3]. However, there is a definite familial and racial tendency to mandibular prognathism. In the United States true skeletal Class III malocclusions are found in less than 1% of the general population[4],[5]. Most orthodontists therefore have much less experience treating patients with Class III malocclusions than they do in treating patients with Class I or Class II malocclusions. For many Class III malocclusions, surgical treatment is the best alternative. Depending on the amount of skeletal discrepancy, surgical correction may consist of mandibular shortening, maxillary lengthening, or a combination of mandibular and maxillary procedures. After surgical correction of the skeletal discrepancy, the occlusion usually can be finished orthodontically in a Class I relationship by using the same principals as in finishing a patient with a nonsurgical Class I relationship. However, if surgical treatment is not performed, and the final molar relationship is Class III, there are challenges specific to the static and functional Class III occlusion that must be considered. The following case report will illustrate some of these challenges and how to deal with them.
Case Report
A female patient of 22 years reported to the department of orthodontics modern dental college and research center, Indore with the chief complain of forwardly placed teeth.
 | Fig 1 Extra Oral Front And Profile With Smiling Photos
 |
Patient History
Medical. There is no relevant medical history. She was a healthy with no systemic disease.
Dental. She had received regular dental care. Her oral hygiene was good. No caries were present, and all restorations were in good condition. There is no history of previous dental treatment.
Extra oral examination
She has mesoprosopic, approximately bilaterally symmetrical facial form with straight profile. Lips were incompetent, acute nasolabial angle and deep mentolabial sulcus. [Fig 1]
Smile Analysis
Non consonant smile arch with increased gingival display. [Fig1]
Intraoral examination
Permanent dentition is present with missing lower lateral incisors and upper third molars. Oval shaped, bilaterally symmetrical upper and lower arch. In centric occlusion (CO) molar and canine relationships were Class III, and the upper incisors were proclined with increased overjet. Spacing present with upper incisors and mild crowding with lower anteriors . Lower midline is shifted towards left and exaggerated curve of spee. [Fig.2]
Radiographic evaluation
OPG reveals missing lower lateral incisors and upper third molars. And convergent roots of lower central incisors. [Fig 3]
Pre treatment cephalometric findings: [Fig 4]
It is a case of skeletal class I relation with horizontal growth pattern. Proclined maxillary dental readings with normally placed lower incisors and soft tissue show normal facial relation[6]
Treatment objectives
1. To establish Class I canine relationship.
2. To eliminate maxillary anterior spacing.
3. To eliminate mandibular anterior crowding.
4. To reduce overjet.
5. To align arches including midlines.
6. To establish a proper incisal guidance
7. To achieve consonant smile arch.
8. To achieve lip competency.
Treatment plan
The following treatment plan was established:
1. Establish Class III molar and Class I canine relationship.
2. Maxillary and mandibular fixed appliances (pre-adjusted edgewise MBT 0.022)[7].
 | Fig 2 Intraoral Pictures Right, Front, Left, Upper And Lower Arch
|
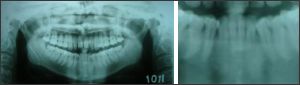 | Fig 3 Opg Reveals Missing Lower Lateral Incisors
|
 | Fig 4 Pretreatment Lateral Cephalogram
|
 | Fig 5 Shows Initial Wire Placement And Transpalatal Arch With Upper Arch For Anchorage Reinforcement
|
 | Fig 6 Intrusion And Retraction With Utility Arch
|
 | Fig 7 Final Settling
|
 | Fig 8 Post Treatment Intraoral Photographs. Lower Canines And Premolars Are Re-contoured As Lateral Incisor And Canine Respectively.
|
3. Converting lower canines into lateral incisor and 1st premolar into canine.(placing canine bracket on 1st premolar and lateral incisor bracket on canines)
4. Initial leveling and alignment with round arch wires. [Fig 5]
5. Proximal stripping in lower anteriors.
6. Intrusion and retraction of upper incisors with utility arch. [Fig 6]
7. Evaluate root alignment after space closure.
Treatment Progress
The appliances were cemented with specific alteration in bracket placement. Initial alignment and decrowding with proximal stripping and rotational wedges proceeded smoothly and without complication within 6 months. After we reach rectangular wire in upper arch utility arch of 17x25 TMA wire was used for retraction and intrusion for next 8 months . Class I canine and Class III molar relationships were established. Final root alignment and settling took another 3 months. [Fig. 7]
Patient cooperation and compliance were good. Fixed appliance treatment was completed in 17 months. Occlusal equilibration was done before and after appliance removal to provide improved contact. Restorative reshaping of lower canine and premolar done after appliance removal. [Fig 8] & [Fig 9]
Treatment Results
The treatment plan was a satisfactory, and the treatment objectives were achieved A Class I canine relationship was established with good alignment. A good overjet was established, midline were coincidinding. Good profile with consonant smile was achieved.
References
1. Angle EH. Treatment of Malocclusion of the Teeth and Fractures of the Maxillae, Angle’s System. 6th ed. Philadelphia, Pa: SS White Dental Manufacturing; 1900:5–15.
2. Prof@257;t WR. Contemporary Orthodontics. St Louis, Mo: CV Mosby; 1986:47–49.
3. Litton SF, Ackerman LV, Isaacson RJ, Shapiro B. A genetic study of Class III malocclusion. Am J Orthod Dentofacial Orthop. 1970;58:565–577.
4. Kelly JE, Sanchez M, Van Kirk LE. An Assessment of theOcclusion of the Teeth of Children. Washington, DC: National Center for Health Statistics, US Public Health Service,1973; DHEW publication no. (HRA) 74-1612.
5. Kelly J, Harvey C. An Assessment of the Teeth of Youths12–17 Years. Washington, DC: National Center for HealthStatistics, US Public Health Service; 1977; DHEW publication no. (HRA) 77-1644.
6. Alex Jacabson .Introduction to radiographic Cephalometry.lea Fesiger;Philadelphia
7. McLaughlin RP, Bennett JC, Trevisi .Systematized orthodontic treatment mechanics. Second Edition. H Mosby International Ltd. |