Introduction
Recent advances in dentistry provide the opportunity for patients to maintain a functional dentition for lifetime. Therapeutic measures performed to ensure retention of teeth vary in complexity. The treatment may involve combining restorative dentistry, endodontics and periodontics so that the teeth are retained in whole or in part. Such teeth can be useful as independent units of mastication or as abutments in simple fixed bridges.The term tooth resection denotes the excision and removal of any segment of the tooth or a root with or without its accompanying crown portion[1].
Various resection procedures described are: root amputation, hemisection, radisection and bisection. Root amputation refers to removal of one or more roots of multirooted tooth while other roots are retained. Hemisection denotes removal or separation of root with its accompanying crown portion of mandibular molars. Radisection is a newer terminology for removal of roots of maxillary molars. Bisection / bicuspidization is the separation of mesial and distal roots of mandibular molars along with its crown portion, where both segments are then retained individually[1].
Weine[1] has listed various indications for tooth resection including: Severe vertical bone loss involving only one root of multi-rooted teeth, Through and through furcation destruction, Unfavorable proximity of roots of adjacent teeth, preventing adequate hygiene maintenance in proximal areas, Severe root exposure due to dehiscence.From a restorative standpoint, treatment by hemisection is indicated for failure of an abutment within a fixed prosthesis, provided a portion of the tooth can be retained to act as the abutment for the prosthesis. Other indications include vertical root fracture confined to a single root of a multirooted tooth or any severe destructive process that is confined to a single root, including caries, external root resorption, and trauma.
Case Report
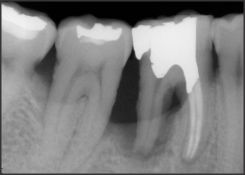
A 35 years old male patient reported with the complaint of pain and mobility in left lower posterior region of mouth. On examination, the mandibular first molar was sensitive to percussion and revealed grade II mobility. The tooth was associated with fractured amalgam filling. On probing the area, there was 8-9 mm deep periodontal pocket around the distal root of the tooth. On radiographic examination,severe vertical bone loss was evident surrounding the distal root and involving the furcation area. The alveolar bone support of mesial root appeared to be adequate (Fig. I).
 | Fig. I : Pre operative Radiograph
 |
Treatment options for such furcation involvement include:
1. Scaling and root planning;
2. Flap curettage;
3. Guided tissue Regeneration and
4. Resective surgery.
First two options were not favored as in both the plans, unhealthy subgingival tissue will definitely be eliminated but residual pocket could have encouraged food lodgment with gingival repair leading to recurrent infection. Guided tissue regeneration was not considered because deeper extension of root caries could have interfered with bone growth at that area up to the desired level. So, it was decided that the distal root should be hemisected after completion of endodontic therapy of the tooth.The tooth so treated would act as abutment for effective prosthetic rehabilitation.
The working length was determined and biomechanical preparation using step back technique was done within the mesial root only. The mesial canals were obturated with lateral condensation method (Fig II) and the chamber was filled with amalgam to maintain a good seal and allow interproximal area to be properly contoured during surgical separation. Under local anesthesia, full thickness flap was reflected after giving a crevicular incision from first premolar to second molar. Upon reflection of the flap, the bony defect along the distal root became quite evident. Curettage was performed to remove chronic inflammatory tissue. The vertical cut method was used to resect the crown. A long shank tapered fissure carbide bur was used to make vertical cut toward the bifurcation area. A fine probe was passed through the cut to ensure separation. The distal root was extracted and the socket was irrigated adequately with sterile saline to remove bony chips and amalgam debris (Fig III).
The furcation area was trimmed to ensure that no spicules were present to cause further periodontal irritation. Scaling and root planning of the root surfaces, which became accessible on removal of distal root was done. The extraction site was irrigated and debrided and the flap was then repositioned and sutured with 3/0 black silk sutures. Subsequently a periodontal pack was applied. The occlusal table was minimized to redirect the forces along the long axis of the mesial root (Fig IV). Patient was called after one week for suture removal and post surgical check up.
After healing of the tissues, an alternative prosthesis (inlay supported- metal ceramic crown involving metal ceramic crown on retained mesial half and class II inlay as retainer on mandibular second molar) was given (Fig V to Fig VIII).
 | Fig. II : Radiograph showing obturation of the mesial root after cleaning and shaping.
|
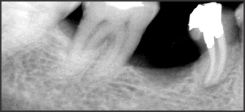
 | Fig. III: Extracted fragment (Distal root)
|
 | Fig. IV: Radiograph showing retained mesial portion
|
 | Fig. V: Tooth preparation done
|
 | Fig. VI: Alternative Prosthesis
|
 | Fig. VII: Prosthesis Seating and Cementation done
|
 | Fig. VIII: Postoperative Radiograph (2 months)
|
Discussion
Success of root resection procedures depend, to a large extent, on proper case selection. It is important to consider the following factors before deciding to undertake any of the resection procedures[5].
Advanced bone loss around one root with acceptable level of bone around the remaining roots.
Angulation and position of the tooth in the arch. A molar that is buccally, lingually, mesially or distally titled, cannot be resected.
Divergence of the roots - teeth with divergent roots are easier to resect.
Closely approximated or fused roots are poor candidates. Length and curvature of roots - long and straight roots are more favourable for resection than short, conical roots.
Feasibility of endodontics and restorative dentistry in the root/roots to be retained.
Hemisection has been used successfully to retain teeth with furcation involvement. However, there are few disadvantages associated with it[1], [2], [8]. It can cause pain and anxiety, more susceptibility to caries especially at the site of hemisection , an improperly shaped occlusal contact area may convert acceptable forces into destructive forces and predispose the tooth to trauma from occlusion.[3]
The present case was treated with an alternative prosthesis (inlay supported- metal ceramic crown involving metal ceramic crown on retained mesial half and class II inlay as retainer on mandibular second molar). Inlay as retainer used in the present case being more conservative preparation restores periodontal health and causes less pulpal damage. In comparison to inlay preparation, full crown causes more damage to vital tissues and improper gingival margins might worsen the periodontal health.
Hemisection has been used successfully to retain teeth with furcation involvement. Hemisection may be a suitable alternative to extraction and implant theapy and should be discussed with patients during consideration of treatment options[7]. Hemisection allows for physiologic tooth mobility of the remaining root, which is thus a more suitable abutment for fixed partial dentures than an osseointegrated counterpart[6].
The smaller size of the occlusal tables, under-contouring of the embrasure spaces and ensuring that the crown margin encompasses the furcation are all factors in the high success rates observed with hemisection therapy [10].
The keys to long term success are thorough diagnosis, selection of patients with good oral hygiene and careful surgical and restorative management[8]. The large variation in success and failure reported by different authors is a reflection that roots resection and hemisection is a technique sensitive procedure[9]. One must be careful throughout the processes of case selection, and endodontic, periodontal, restorative and maintenance therapies.
Conclusion
The prognosis for hemisection is the same as for routine endodontic procedures provided that case selection has been correct, the endodontics has been performed adequately, and the restoration is of an acceptable design relative to the occlusal and periodontal needs of the patient. Hemisection should be considered as an important weapon in the squad of dental surgeon. With increasing desire to retain natural teeth, various different procedures were routinely followed for periodontally diseased teeth and hemisection has received acceptance as a conservative and dependable dental treatment.
References
1. Weine FS. Endodontic Therapy, 5th Edition.
2. Ingle JI and Bakland LK. Enddodontics, 5th Edition.
3. William F. Ammons, Jr., Gerald W. Harrington. chapter 68 – Furcation: Involvement and treatment. Carranza’s Clinical Periodontology, 10th edition, 991-1004.
4. Kost WJ, Stakiw JE. Root amputation and hemisection J. Canad Dent Assoc1991; 57: 42-45.
5. Parmar G,Vashi P. Hemisection: a case-report and review. Endodontology. 2003; 15:26-29.
6. M. Najeeb Saad, Jorge Moreno, Cameron Crawford. Hemisection as an Alternative Treatment for Decayed Multirooted Terminal Abutment: A Case Report. JADC june 2009, Vol. 75, No 5, 387-390.
7. Sunandan Mittal , Tarun Kumar , Ramta Bansal , Dilpreet Kaur: Hemisection As An Alternative Treatment For Decayed Multirooted Tooth, Indian Journal of Dental Sciences; 08-09.
8. Pradeep Shukla, Deepak Grover. Hemisection- A Case Report. JIDA. 2010;4(12):597-8
9. Vaibhavi Joshipura. Hemisection- A relevant, practical and successful treatment option. JIOH :2011;3(6):43-48
10. Savitha Akki, Sudhindra Mahoorkar. Tooth Hemisection and Restoration an Alternative to Extraction- A Case Report. International Journal of Dental Clinics 2011:3(3):67-68
11. Vineet S. An innovative approach for treating vertically fractured mandibular molar - hemisection with socket preservation. Journal of Interdisciplinary Dentistry. 2012;2(2):142-143. |