Introduction
The transition from the deciduous to the permanent dentition is a complex process rich in details and represents one of the nature's expressions of perfection. However, as all natural processes, the dental development can show some face irregularities: The dental anomalies. Dental anomalies are the formative defects caused by genetic disturbances or environmental factors during tooth morphogenesis. Dental anomalies are the formative defects caused by genetic disturbances or environmental factors during tooth morphogenesis. Developmental defects occur either alone or in combination with other birth defects.
Microdontia is a rare phenomenon. The term microdontia (microdentism, microdontism) is defined as the condition of having abnormally small teeth[1]. According to Boyle, "in general microdontia, the teeth are small, the crowns short, and normal contact areas between the teeth are frequently missing". [2] According to Shafer microdontia are of three types[3]: (1) Microdontia involving only a single tooth (2) relative generalized microdontia due to relatively small teeth in large jaws and (3) true generalized microdontia, in which all the teeth are smaller than normal. Microdontia of a single tooth can be further classified into (1) microdontia of the whole tooth, (2) microdontia of the crown of the tooth, and (3) microdontia of the root alone[4]. The most common teeth affected are maxillary lateral incisor and third molar[5].
The functional and aesthetic changes caused by microdontia impose the necessity of finding a therapeutic approach of shaping the permanent dentition in a way that normal occlusal relationships and improved aesthetics could be achieved. This article is related to the nature's errors applied to dental development and discusses the accurate diagnosis as well as therapeutic approach to anomaly.
Case Report:
The patient was a 27 year old male reported to the out patients department with the complaint of small teeth. Patient noted small teeth ever since the eruption of permanent teeth. No abnormalities were reported, however, in their family.
Physical Examination
Physical growth was within normal limits. The patient was normal in stature, appearance, height, and weight from his age. No abnormality was noted in neck, back, muscles, cranium and joints as well upon other examination like that of the limbs, hands, skin, hair, nails and eyes were all appeared normal.. Intellectual performance was also normal. His medical history was unremarkable; no other abnormalities were noted in the history as well. The child was examined and found to be free of any gross abnormalities. His blood profile was normal. Serum calcium, phosphorous and alkaline phosphatase levels were also normal. Endocrinological investigation was carried out to rule in or out the possibility of hormonal disorder, and the results were within normal limits.
Extraoral Examination:
Extra oral examination did not reveal any abnormality.
Intraoral Examination:
Intraoral examination reveals permanent dentition with class I molar relationship with Soft tissues appearing normal in color and contour. Hard tissue examination revealed undersized left central incisor (21) compared to adjacent
 | Figure 1: Photograph showing microdontia of left central incisor
 |
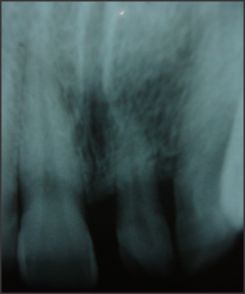 | Figure 2: Intraoral radiograph showing undersized crown and root of left central
|
right central incisor. The crown of 21 also showed slender indentation on right side. (Figure1). Diagnostic cast was obtained to aid in diagnosis.
Radiographic Examination:
Radiographic examination was carried out which reveal reduction or small size of root of left central incisor as compared to adjacent right central incisor which confirmed the diagnosis. (Figure 2)
Diagnosis:
A diagnosis of non-syndromic occurrence of true localized microdontia of maxillary central incisor (single tooth) involving both crown as well as root was made as no systemic condition was observed. The conservative management is advised for microdontia keeping in mind the age, sex of the patient, crown length, crown root ratio etc. An interim porcelain crown was given to patient.
Discussion:
Developmental dental anomalies are an important category of dental morphologic variations. Abnormalities in tooth size, shape, and structure result from disturbances during the morpho-differentiation stage of development, while ectopic eruption, rotation and impaction of teeth result from developmental disturbances in the eruption pattern of the permanent dentition.[6] Their incidence and degree of expression can provide important information for phylogenic and genetic studies and help in the understanding of differences within and between populations.[7]
Tooth size is variable among different races and between the sexes. When teeth in both arches are smaller than normal is termed as generalized microdontia. If all teeth are uniformly smaller than normal as seen in pituitary dwarfism, the condition known as true generalized microdontia. The term relative generalized microdontia is used when both arches are somewhat larger than normal but the teeth are of normal size, giving illusion of generalized microdontia.[8] One of the most common localized microdontia is peg lateral and root of such tooth is also shorter than usual but tooth affected in present case is very rare. Very few literature shows true microdontia of central incisor.[5],[9] It was noted that anomalies were more frequent in male patients than in females.[10]
Microdontia occurred more frequently in the maxillary teeth than the mandibular. The prevalence of microdontia in southern Chinese children was 6.3% which was much higher than for other ethnic groups.[11] The prevalence of peg-shaped teeth reported by Clayton[12] and Saito[13] were 0.2%. The prevalence of this condition ranges from 0.8% to 8.4% in various populations[9] in 2005, 2010 prevalence rate was reported to be 9.14% of total anomalies with a majority of peg shaped lateral incisors[10] and 2011 it was reported to be 2.58%.[14]
An autosomal-dominant inheritance pattern has been associated with this condition.[15]. The initiating factor or factors responsible for microdontia remain obscure. Mutation in developmental regularity genes are known to cause variety of dental defects.[16] Both genetic and environmental factors are involved in the complex etiology of microdontia. Genetic factors probably play a role in the formation of microdontia[17]
The development of a tooth has been shown to have neural crest, ectodermal and mesodermal contributions. The variation in size of a particular tooth arises during the period when the form of the tooth is being determined by the enamel organ and the hertwig epithelial sheath at the bell stage of enamel organ of tooth development. The determination of the form of the crown is thought to be related to different regions of the oral epithelium or to the ectomesenchyme. Studies have shown that different regions of the oral epithelium rather than the underlying ectomesenchyme are initially responsible for the shape of the crown.[18]
The syndromes associated with microdontia are Gorlin-Chaudhry-Moss syndrome, Williams's syndrome, Chromosome d/u, 45X [Ullrich-Turner syndrome], Hallermann-Streiff, Chromosome 13[trisomy 13], Orofaciodigital syndrome (type 3), Rothmund-Thomson syndrome, Oculo-mandibulo-facial syndrome, Tricho-Rhino Phalangeal, type1 Branchiooculo- facial syndrome.[19]
As the patient did not show any abnormal systemic manifestations, all the syndrome associated with the dental anomalies were ruled out. The presence of small maxillary central incisor in which both crown as well as root is affected is rare. To our knowledge only few literatures reported such unusual nature of dental anomaly of non-syndromic occurrence of true microdontia in association with abnormality in shape of tooth.
Conclusion:
Developmental anomalies of teeth are clinically evident abnormalities. They may be the cause of various dental problems. Careful observation and appropriate investigations are required to diag-nose the condition and institute appropriate treatment.
Refrences:
1. Laundau S: International dictionary of medicine and biology. New York: John Wiley & Sons;, 1 1986, 1717.
2. Boyle PE: Kronfeld's Histopathology of the Teeth and their Surrounding Structures. Philadelphia: Lea& Febiger; 3 1955, 14.
3. Shafer WG, Hine MK, Levy BM: A Textbook of Oral Pathology. Philadelphia: W. B. Saunders Co;, 1 1958, 26.
4. Ufomata D: Microdontia of a mandibular second premolar. Oral Surg Oral Med Oral Pathol 1988; 65:637-8.
5. Sharma A. Unusal localized microdontia: Case Report. J Indian Soc Pedo Prev Dent 2001 ;19: 1:38-39
6. Proffit WR. The development of orthodontic problems. In: Contemporary orthodontics, 2nd ed, Proffit WR ed, Mosby, St Louis, 1997;110
7. Bailit HL. Dental variation among populations. An anthropologic view. Dent Clin North Am 1975; 19, 125-139.
8. Sapp JP, Eversole LR, Wysocki GP. Contemporary Oral & Maxillofacial Pathology. 2nd ed.Mosby: 2004;1-2
9. Neville DW, Damm DD, Allen CM, Bouquot JE. Abnormalities of teeth. In: Oral and Maxillofacial Pathology. 2nd ed. Philadelphia, PA: Elsevier; 2005:49-89.
10. Kruthika S Guttala , Venkatesh G Naikmasurb, Puneet Bhargavac , Renuka J Bathid. Frequency of Developmental Dental Anomalies in the Indian Population. European Journal of Dentistry 2010;4 263-69
11. Nigel M. King, S. Tongkoom and H.M. Wong Morphological and Numerical Characteristics of the Southern Chinese Dentitions. Part III: Anomalies in the Primary Dentition. The Open Anthropology Journal, 2010; 3: 25-36
12. Clayton JM. Congenital dental anomalies occurring in 3357 children. J Dent Child 1956; 23: 206-8
13. Saito T. A genetic study on the degenerative anomalies of deciduous teeth. Jap J Hum Genet 1959; 4: 27-53
14. Saurabh K. Gupta, Payal Saxena1, Sandhya Jain and Deshraj Jain. Prevalence and distribution of selected developmental dental anomalies in an Indian population. Journal of Oral Science2011;53(2):231-238,
15. Regzi JA, Sciubba JJ, Jordan RCK. Oral Pathology:Clinicopathoogical correlation.4th ed.Saunder; 2003:367
16. Thesleff I: Genetic basis of development of dental defects. Acta Odontol Scand 2000; 58:191-4.
17. Bargale and Kiran: Non-syndromic occurrence of true generalized microdontia with mandibular mesiodens - a rare case. Head & Face Medicine 2011; 7:19.
18. Osborn JW, Ten Cate AR: Advanced dental histology: dental practitioner. Handbook no, 6. Bristol: John Wright & Sons 1976; 3:24-51.
19. Seema D Bargale and Shital DP Kiran. Non-syndromic occurrence of true generalized microdontia with mandibular mesiodens - a rare case. Head & Face Medicine 2011, 7:19 |