Introduction:
Primary impaction of primary teeth is rare. [1], [2], [3], [4]. A tooth that fails to erupt in the oral cavity and achieve normal functional position by the time it should normally erupt is considered as impacted. These impacted teeth tend to be asymptomatic and are found on routine radiographic examination when the patient is in the mixed dentition or permanent dentition stage. Ravnn[5] studied the numerical variations and fusions in the primary dentition among 4,564 children from 3 to 3½ years of age. The results showed that aplasia occurs in 0.5%, hyperodontia in 0.5%, and fusions in 0.9%. Patients with aplasia in the primary dentition nearly always showed aplasia of the successors. In patients with unilateral aplasia in the primary dentition, aplasia of the contralateral permanent tooth was often found also[5]. Prolonged impaction of primary incisors is unusual. Prolonged impaction of the maxillary primary left lateral incisor was associated with eruption delay, ectopic eruption, and an apparent dilaceration of the root of the maxillary left permanent lateral incisor[6].
Case Report:
A 9-year, 1-month-old, 56-1b girl appeared for an initial examination with the chief complaint of non-eruption of the upper front teeth (Fig 1). The parents told that the maxillary primary incisors had never erupted, which heightened concern about the status of the maxillary permanent incisors. However, there was no additional abnormality in the anterior maxillary region. Both parents stated that the maxillary
 | Fig 1. Intra-oral Preoperative View Shows Unerupted Primary Incisors.
 |
 | Fig 2. Opg Showing Unerupted Primary Incisors.
|
primary incisors had not been lost prematurely and, in fact, had never erupted. The child was the product of an uncomplicated full-term pregnancy and was healthy otherwise. The child was brought up under good maternal care till date and never had any traumatic injury that to cause intrusion or the loss of the primary anterior teeth. Both the OPG and the maxillary occlusal radiographs showed impacted primary incisors
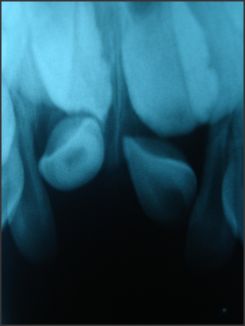 | Fig 3. Maxillary Occlusal View Showing Impacted Primary Incisors.
|
(Fig 2(a) & Fig 2(b). Removal of primary maxillary impacted incisors was planned and these were removed (Fig 3, 4, 5). The patient was put on follow-up. After a period of 2 years the permanent incisors erupted (Fig 6). The right upper central
 | Fig 4 (A).extracted Primary Incisors Viewed From Apical.
|
 | Fig 4 (B). Extracted Primary Incisors Viewed From Front.
|
 | Fig 5.intra-oral View After Removal Of Impacted Primary Incisors.
|
{Image 7]
incisor was malformed and hypoplastic, whereas the left one showed normal formation.
Discussion:
The case presented here shows the malformed and impacted primary maxillary incisors. The prevalence of impacted primary teeth has been reported to be very rare and was reported to occur in 1:10,000 times, most commonly involving the primary second molars[3]. Aizenbud et al[7] presented a case of an unerupted malformed primary central incisor, histologically diagnosed as a compound odontoma. Zengin et al[8] suggested the influence of genetic factors in the occurrence of tooth agenesis and primary impacted teeth in monozygotic twins. Qin M et al[9] found disturbances of dentin mineralization, hypoplasia or aplasia of root cementum and external resorption of root dentin as causative factors for impaction and the hypoplasia or aplasia of root cementum was thought to be the prime etiological factor in the early loss of primary teeth and in the present case report the extracted teeth showed similar malformation and hypoplasia of roots.
Studies have shown that when the primary teeth are absent there is a high prevalence of the absence of succedaneous teeth [8]. Ravn[5] reported that patients with aplasia in the primary dentition showed a similar pattern in the permanent dentition in 80% of the cases. Disturbances in primary dentition can affect the permanent teeth to varying degrees.The topographic relationship of the primary teeth to the permanent tooth germs explains the potential for possible developmental disturbances[10].The developmental defects of the permanent successor tooth ranges from mild alteration in enamel mineralization in form of simple white or yellow brown discoloration to crown dilacerations, crown duplication, root dilaceration, root duplication, odontome like malformation, partial or complete arrest of root formation to severe sequestration of the developing tooth germ[11],[12]. Kapur A et al[3]discussed the presence of impacted inverted maxillary primary incisors and their management by surgical intervention in a 5 year old boy. It is important for paediatric dental surgeons to carefully monitor the eruption of primary and permanent teeth for early identification and management of developmental anomalies. Therefore, we should carefully inspect for the impacted primary and permanent teeth for early identification and proper management.
References:
1. Bianchi SD, Roccuzzo M. Primary impaction of primary teeth: a review and report of three cases. J Clin Pediatr Dent. 15(3):165-8, 1991.
2. Lambert M, Rothman DL. Unusual impaction of a primary lateral incisor. ASDC J Dent Child. 61(2):146-8, 1994.
3. Kapur A, Goyal A, Jaffri S. Management of inverted impacted primary incisors: An unusual case. J Indian Soc Pedod Prev Dent. 26:26-8, 2008.
4. Darwish SM, Salama FS: Impacted primary mandibular central incisors: case report. J Clin Pediatr Dent. 26(4):347-9, 2002.
5. Ravnn, J. J. Aplasia, supernumerary teeth and fused teeth in the primary dentition. European Journal of Oral Sciences, 79: 1-6, 1971.
6. Timothy W. Adams, An impacted primary lateral incisor as a cause of delayed eruption of a permanent tooth: case report. Paediatric Dentistry 20:2, 1998.
7. Aizenbud D, Front Y P. An impacted malformed primary maxillary central incisor diagnosed as a compound odontoma. The Journal of clinical pediatric dentistry. 33(2): 161-165, 2008.
8. Zengin Z A, Sumer P A, and Karaarslan E. Impacted Primary Tooth and Tooth Agenesis: A Case Report of Monozygotic Twins. Eur J Dent. 2: 299-302, 2008.
9. Qin M, Shi G, Ge L. A light and scanning electron microscopic study of primary teeth in hypophosphatasia. Zhonghua Kou Qiang Yi Xue Za Zhi. 34(4):220-2, 1999.
10. Kalra N. Sequlae of neglected pulpal infections of deciduous molars.Endodontology; 19-23, 1994.
11. Stewart D J.Dilacerated unerupted maxillary central incisor.Br Dent J ; 145:229-33,1978.
12. Turner J O. Two cases of hypoplasia of enamel.Br J Dent Sci. 55; 227-8,1912. |