Background
Gingival overgrowth is among one of the most important clinical features of gingival pathology. It has multifactorial etiologies and has been frequently associated with inflammatory changes. Other factors related to the condition are hereditary (familial), malignancies and those resulting from adverse effects associated with the systemic administration of certain drugs[1]. Prevalence of drug induced gingival enlargement is 3-20% compared to most important inflammatory gingival enlargements[2]. Clinical manifestations of gingival enlargements frequently appear within 1-3 months, after initiation of treatment with the associated medication. It begins with enlargement of the interdental papilla which is normally confined to the attached gingiva but may extend coronally. Gradually gingival lobulations may form, appearing inflamed or fibrotic, and is most frequently found in the anterior segment of the labial surfaces, which grows outwardly and may cover the labial surfaces of the teeth partially. It may be associated with secondary inflammatory changes. We report a peculiar case of non regressive amlodipine induced gingival overgrowth confined only to the incisive papilla[1],[2].
Case discription
A 52 years old male patient came to the department of Periodontics HP govt. Dental College and Hospital Shimla (HP) with the chief complaint of annoying nodule on the palatal side of the mouth. Patient was aware of the growth for last 4 years and was seeking medical attention. He first noticed a small bead like nodule on the front palatal side that gradually progressed to the present size covering almost the palatal surfaces of upper central incisors. Enlargement was not associated with bleeding or loosening of teeth. His past medical history revealed that the patient was hypertensive and was under medication for last 10 years (amlodipine 5 mg once daily), however his past dental history was non contributory. (Fig-1)
The haemogram of the patient was found
 | Fig-1 : (Showing Enlarged Incisive Papilla)
 |
to be under normal range. Ortho pantomogram revealed complete set of dentition with generalized bone loss. Based on history and clinical and radiographic picture the provisional diagnosis of drug induced gingival enlargement was made. The treatment of
 | Fig-2 : (Biopsy Sample Sent For Examination)
|
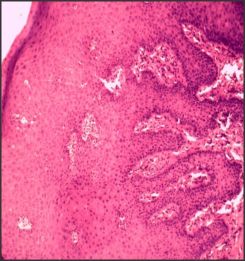 | Fig-3 (a) Histopathologic Slide Showing Enlarged Rete Ridges And Epithelial Proliferation.
|
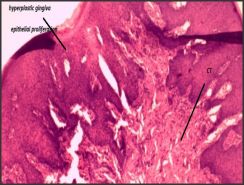 | Fig-3 (b) Connective Tissue Is Made Of Dense And Loose Fibrous Components And Inflammatory Cell Infiltrate.
|
the patient was started with non surgical approach which included phase -I therapy with planned sessions of scaling and root planing. Simultaneously patient's physician was consulted regarding drug substitution or withdrawal of the drug. The physician substituted drug with Labetalol 100mg once daily. Patient was instructed to maintain good oral hygiene with the use of chlorohexidine oral rinses 0.12%.
After drug substitution and maintenance of regular oral hygiene for 3 months there was only a minimal regression in the size of gingival enlargement with maximum of fibrotic component left. Therefore a gingivectomy procedure was planned. (Fig-2)
Finally excisional biobsy of the gingival hyperplastic nodule was done under LA (plain lignocaine 2%). Biopsy sample size 5x5 mm was obtained and preserved in 10% formalin solution in a sterile vial. Histopathological report revealed mixture of dense and loose fibrous components with inflammatory cell infiltrate in the connective tissue. Epithelium showed acanthosis and elongation of rete apexes. On the basis of patient's history, clinical features and biopsy reports, a diagnosis of amlodipine induced gingival overgrowth (AIGO) was made. The post operative results were found to be extremely satisfactory both esthetically and functionally. (Fig-3a, Fig-3b)
Discussion
The prevalence of gingival growth induced by chronic medications such as calcium channel blockers is uncertain, although there have been several studies with confiscatory results[2]. The prevalence of clinically significant overgrowth related to nifedipine is around 30%[3] and amlodipine is around 1.7-3.3%[4]. Males are 3 times more likely to develop the overgrowth[4],[5]. Gingival inflammation is an important cofactor for the expression of effects. Dose dependent correlation with the severity of gingival overgrowth is weak, but decrease drug use, in general, results in reduced severity of gingival pathology. Genetic predisposition is among the additional risk factors[6].
Despite their pharmacological diversity all three forms of drugs (antihy pertensive, antiepileptic, immuno suppressants) responsible for gingival enlargements have similar mechanism of action at cellular level, where they all inhibit intracellular calcium ion influx. The action of these drugs may prove to be the key to understanding that why all the three drugs have common side effect on secondary target tissue (gingiva) [7]. Histological and clinical picture of overgrowth associated with all the three categories of drugs also found to have common characteristic. Efforts have been made to find a proposed hypothesis for the etiology behind drug induced gingival enlargements:-(a)it is hypothesisized that the individuals with an abnormal susceptibility to drugs have more gingival enlargements.(b)role of inflammatory cytokines:-a synergistic enhancement of collagenous protein was found to be elevated when these cells are simultaneously exposed to nifedipine, a proinflammatory cytokine that is found to be elevated in addition to IL-1,Il-2,Il-6.(c)role of MMP'-these drugs may interfere with the synthesis and the degeneration of collagen by blocking MMP synthesis by decreasing the calcium influx[8],[9].
Efforts should be made to increase the awareness about drug induced gingival enlargements in the community. The clinician should emphasize the importance of detailed medical history of the patient including the history of epilepsy, cluster headache (for which patient takes verapamil)[7],[10],[11] history of renal transplants and kidney dialysis. The clinician should emphasize plaque control as the first step in the treatment[2]. Usually a three month interval for periodontal maintenance therapy has been recommended after the substitution or cessation of drug in such patients. Confirmatory biopsies should be taken to establish a definitive diagnosis for drug induced gingival enlargements and to rule out the other possibilities of gingival enlargements like myeloid sarcoma[12]. Early identification of patient susceptible to drug induced overgrowth will help minimize the treatment needed to control the entity.
Conclusion
This case further highlights the role of amlodipine in gingival enlargements.So far only the labial gingival enlargements has been reported to be drug induced, here we report a case of amlodipine induced enlargement at gingival papilla which is a rare site. In our thorough search of literature we could find no such report, hence this report is probably one of the first reported cases. we futher emphasize the importance of biopsy examination for the confirmation of results in every such cases.
Clinical Significance
As amlodipine is a commonly prescribed drug in routine practice, every physician should be aware of its usually overlooked but harmful side effects, particularly if adverse oral symptoms arise during drug use. Biopsy should be taken for every case to make out a definitive diagnosis.
References
1. Text book of clinical Periodontology, edi 10, Michael G. Newman, Henery H. Takei, Perry R. Klokkevold, Fermin A. Carranza:
2. Amlodipine induced gingival overgrowth, M.G. Triveni, C. Rudrakshi, D.S. Mehta, J Indian Soc Periodontal.2009 Sep-Dec;13(3):160-163.
3. Lncidence of gingival hyperplasia caused by calcium antagonists in continuous ambulatory peritoneal dialysis patients, Junko Shouda et al, J Clin Periodontal 2004;31:126-131.
4. Amlodipine induced massive gingival hypertrophy, Murat Sucu, Vedat davutoglu, Canadian family physician 2011;57.
5. Prevalence of gingival overgrowth induced by calcium channel blockers :A Community based study, Janice S.Ellis, Journal of Periodontology Jan 1999;70(1): 63-67.
6. Prevalence of risk of gingival enlargement in patients treated with nifepine, Jaume Miranda, Journal of periodontology, Jan 2004; 69(1):88-99.
7. The role of drugs in pathogenesis of gingival overgrowth, William W. Hallmon & Jeffery A.Rossman , periodontal 2000;(70):256-60.
8. Conservative management of nifedipine influenced gingival enlargement-A case report,Natasha Attri, Sunil Mahajan, Harinder Gupta, 2012;4(1).
9. Gingival overgrowth in children:epidemiology, pathogenesis and complications. A literature review,Aikaterini Doufexi et al, journal of periodontoly, Jan 2005;76(1): 3-10.
10. Virapamil induced gingival enlargement in cluster headache,MS Matharu,J a Van Vliet, M.D Ferrari, J Neurol Neurosurg Psychiatry 2005 ;76:124-127.
11. Amlodipine induced gingival hyperplasia, Ardeshir Lafzi et al, Med Oral Patol Oral Cir buccal 2006;11:E 480-2.
12. Myeloid sarcoma occurring concurrently with drug induced gingival enlargement,Angela J.Yoon et al, Journal of periodontology; jan 2006;77(1) :119-122. |