Introduction
Ameloblastoma is a benign epithelial odontogenic tumor characterized by a local invasiveness and high frequency of recurrence. It includes several clinicoradiographic and histologic subtypes like follicular, plexiform, acanthomatous, basaloid and granular cell types.[1] Eversole et al in 1984, first described Desmoplastic ameloblastoma (DA) in detail.[2] It is defined as "a variant of ameloblastoma with specific clinical, imaging and histological features" in the recent World Health Organization classification of odontogenic tumors.[3] Follicular and plexiform are the commonly encountered variants accounting to 32.5% and 28.2% respectively; followed by the acanthomatous subtype with 12.1% while desmoplastic is extremely uncommon with incidence rates ranging from 4-13% in various reports.[1] DA often occurs in the anterior region of jaws, presents with unique radiographic appearance of mixed radiolucency and radiopacity, resembling fibrosseous lesions. The mixed radiographic appearance is due to osseous metaplasia within the dense fibrous septa that characterizes the lesion, and it is not because of the production of a mineralized product by the tumor. DAs show distinct histopathology characterized by extensive stromal collagenisation or desmoplasia surrounding compressed islands of odontogenic epithelium making it a distinct entity.[4] A possible transitional form of DA showing the microscopic features of the desmoplastic variant together with areas typical of classic follicular or plexiform ameloblastoma has been called a hybrid lesion of ameloblastoma.[1] This article aims to describe a case of DA which occurred in the maxilla of a 60 year-old woman.
Case Report
A 60-year-old female reported to a private clinic with a chief complaint of swelling in the maxillary anterior region since 6 months. It was slow growing and was not associated with pain. Extraoral examination revealed a swelling extending superiorly from the infra-oribital region to the angle of the mouth inferiorly and upto the right ala of nose mesially causing facial asymmetry on the right side of the face (Fig - 1). On intra-oral examination, a well-defined swelling of 6x3 cm was seen in the premaxilla region extending from 14 to 24. Swelling was oval, firm, nontender and was attached to the underlying structures. No surface ulcerations were noticed (Fig - 2). Orthopantomogram showed an unilocular radiolucency of
 | Figure 1 : Extraoral swelling extending superiorly from the infra-oribital region to the angle of the mouth inferiorly and upto the right ala of nose mesially.
 |
 | Figure 2 : Well-defined oval, firm, nontender swelling seen in the premaxilla region extending from 14 to 24.
|
 | Figure 4 : Surgical excision of the lesion.
|
size 5x3 cm with radiopaque flecks within (Fig - 3). The patient was referred to the department of Oral and Maxillofacial Pathology, Kalinga Institute of Dental Sciences. An incisional biopsy was done followed by histopathological examination. The specimen revealed a dense collagen stroma with scattered epithelial islands. The epithelial islands showed peripheral cuboidal cells with nuclear hyperchromatism. Some peripheral cells in the island showed reverse polarity. A diagnosis of desmoplastic ameloblastoma was made. Then the patient was planned for total surgical removal of the lesion under general anaesthesia. The entire mass was found to be well-encapsulated and was enucleated in toto (Fig - 4).
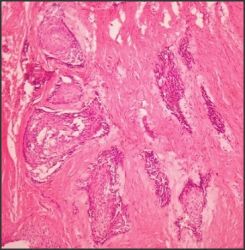
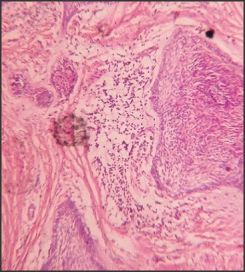
Histopathology of the excised tumor revealed epithelial islands dispersed within a dense collagen stroma. The epithelial islands were irregular and bizarre in shape (Fig - 5). The epithelial cells at periphery of the islands were cuboidal. Few cells exhibited hyperchromatic nuclei. Some areas showed peripheral cells resembling ameloblasts with reverse polarity. Few islands revealed features of acanthomatous ameloblastoma with the central cells showing squamoid appearance and foci of keratinization (Fig - 6). The stroma revealed a moderately cellular fibrous connective tissue with abundant thick collagen fibers. The epithelial islands appeared to be squeezed within the collagen fibers. Myxoid changes of the stroma surrounding a few epithelial islands was seen. Few areas showed features of follicular ameloblastoma with epithelial islands showing central mass of loosely connected angular cells resembling stellate reticulum surrounded by a layer of columnar ameloblast like cells (Fig - 7). A final diagnosis of hybrid desmoplastic ameloblastoma was made. The patient's postoperative course was
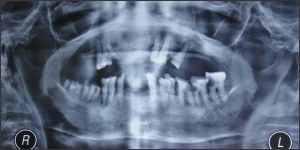 | Figure 3 : Orthopantomogram showing an unilocular radiolucency with radiopaque flecks within.
|
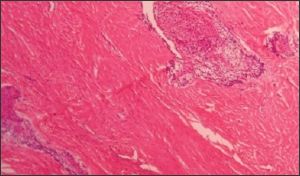 | Figure 5 : Photomicrograph showing epithelial islands dispersed within a dense collagen stroma. The epithelial islands were irregular and bizarre in shape.
|
 | Figure 6 : Histopathology revealing features of acanthomatous ameloblastoma with the central cells showing squamoid appearance and foci of keratinization.
|
 | Figure 7 : Myxoid changes of the stroma surrounding a few epithelial islands was seen. Few areas showed features of follicular ameloblastoma with epithelial islands showing central mass of loosely connected angular cells resembling stellate reticulum surr
|
uneventful. Postoperative radiography and a clinical follow-up examination six months later disclosed no recurrence or residual tumor.
Discussion
Eversole et al in 1984 first described three cases of desmoplastic ameloblastoma.[2] Later, Waldron and El Mofty reported additional 14 cases.[5] It is somewhat new and a rare entity accounting to 4%-13% of all ameloblastomas.[6] The striking difference in the anatomic location i.e. occurrence in the anterior-premolar region of maxilla/mandible, unusual radiologic presentation of mixed radiolucency-radiopacities with ill-defined borders and distinctive histopathology of extensive stromal desmoplasia with scattered odontogenic epithelium makes it a distinct clinicopathologic entity. Additional findings reported for DA are almost equal sex predilection and relative higher frequency of occurrence in Asians.[7] Desmoplastic ameloblastomas was categorized as a distinct variant of ameloblastoma in the World Health Organization classification of odontogenic tumors in 2005.[3] Approximately half of the desmoplastic lesions are located in the maxilla, and the vast majority of them occur in the anterior or premolar portion of the jaws. Maxillary lesions are more insidious than mandibular tumors owing to the proximity of vital structures and the maxillary sinus. Also, the very thin cortical bone of the maxilla forms a weak barrier for the spread of tumors.[8] The radiographic appearance of this neoplasm usually indicates a mixed radiolucent/radiopaque lesion. Approximately half of these lesions have diffuse borders in the radiography and look similar to a fibro-osseous lesion. Takata et al believed that the mixed radiologic appearance expresses the infiltrative pattern of the tumor.[9]
Waldron and El Mofty described the histologic appearance of DA as small ovoid islands and narrow cords of odontogenic epithelium widely separated by dense, moderately cellular, fibrous connective tissue. Spicules of mature lamellar bone trabeculae have been reported in intimate contact with the tumor, and invasion has been demonstrated. This histologic finding may indicate the potential for local invasion, and accounts for the diffuse radiographic imaging.[5] "Hybrid" lesion of desmoplastic ameloblastoma and conventional ameloblastoma is an unusual variant of ameloblastoma, which was first described by Waldron & El Mofty in 1987. Hybrid lesions show typical microscopic features of desmoplastic ameloblastoma characterized by pronounced stromal desmoplasia together with areas of follicular, plexiform and acanthomatous ameloblastoma.[5],[6] The cause for this peculiar histologic appearance is still unclear. Various immunohistochemical studies have reported DA tumor cells as showing variable expression of S-100 protein and desmin, marked immunoexpression of TGF-β, high expression of caspase-3 and Fas, decreased expression of CK19 and high expression of p63.[4] Compared with the stroma of SMA, the desmoplastic stroma of DA has been reported to show a strong positive reaction for collagen type VI,[1] immunonegativity for tenascin, and strong immunopositive reaction for fibronectin and type 1 collagen.[4] Desmoplasia of the stromal connective tissue in DA can be argued to be a maturation of SMA, as similar dense collagenization is seen during maturation of longstanding tumors. This argument can be supported by the existence of 'hybrid' tumors, wherein the follicles are present in a desmoplastic background. But the lesser frequency of DA in the posterior mandible compared with SMA is then unanswered. Firstly, it is probable that the location of the tumor can influence the maturity of the lesion and, hence, the tumors in the anterior jaws may mature sooner than those occurring in the posterior mandible.[4] But according to some authors, it is much too early to speculate whether desmoplastic changes occur secondarily in the stroma of a pre-existing SMA, or whether areas of primary DA transform into a SMA. Hence it has been suggested that the hybrid lesion should be considered a collision tumor.[1]
Many controversies surround the hybrid lesion. The present case showed features of hybrid lesion histologically. The lesion was well encapsulated which was enucleated instead of resecting along with normal margin. Both SMA like areas along with DA areas were seen under microscope leading to a diagnosis of hybrid variant of desmoplastic ameloblastoma. Present case is being closely followed and no evidence of recurrence has been reported till date. Many cases like this should surface in the literature so that the biological behaviour of hybrid lesions will be deciphered and treatment modalities will be planned accordingly.
References
1. Reichart PA, Philipsen HP. Odontogenic tumors and allied lesions. Quintessesnce Publishing Co. London. 2004, 1 st edition; 69-77.
2. Eversole LR, Leider AS, Hansen LJ. Ameloblastomas with pronounced desmoplasia. J Oral Maxillofac Surg.1984; 42: 735-740.
3. Gardner DG, Heikinheimo K, Shear M, Philipsen H P, Coleman H. Ameloblastomas. In: L. Barnes, J.W. Eveson, P Reichart and D. Sidransky, (Eds). World health organization classification of tumors. Pathology and genetics of head and neck tumors. IARC Press, Lyon; 2005.296-300.
4. Yazdi Ismail, Seyedmajidi Maryam, Foroughi Ramin. Desmoplastic Ameloblastoma (a Hybrid Variant): Report of a Case and Review of the Literature. Arch Iranian Med. 2009; 12 (3): 304 - 308.
5. Waldron CA, El Mofty SK. A histopathologic study of 116 ameloblastomas with special reference to the desmoplastic variant. Oral Surg Oral Med Oral Pathol. 1987; 63: 441 - 451.
6. Philipsen HP, Reichart PA, Takata T. Desmoplastic ameloblastoma (including 'hybrid' lesion of ameloblastoma). Biological profile based on 100 cases from the literature and own files. Oral Oncol. 2001; 37: 455 - 460.
7. Punnya. V Angadi, Alka Kale, Seema Hallikerimath, Vijayalakshmi Kotrashetti, Deepa Mane, Pooja Bhatt, et al. 'Hybrid' desmoplastic ameloblastoma: an unusual case report with immunohistochemical investigation for TGF-?. Estern J Med. 2011; 16: 9-17.
8. Kawai T, Kishino M, Hiranuma H, Tadashi S, Ishida T. A unique case of desmoplastic ameloblastoma of the mandible; report of a case and brief review of English language literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87: 258-263.
9. Takata T, Miyauchi M, Ito H, Ogawa I, Kudo Y, Zhao M, et al. Clinical and histopathological analyses of desmoplastic ameloblastoma. Pathol Res Pract. 1999;195(10):669-75. |