|
|
|
| Assessment Of Third Molar Eruption Status Among Students Of Swami Devi Dyal Group Of Professional Institutions, Barwala (panchkula) |
Nidhi Gupta 1 , Mohit Bansal 2 , Shelja Vashisth 3 , Nanak Chand Rao 4
1 Professor, Dept of Public Health Dentistry - Swami Devi Dyal Hospital & Dental College, Golpura, Barwala, Distt. Panchkula, India.
2 Lecturer, Department of Public Health Dentistry, - Swami Devi Dyal Hospital & Dental College, Golpura, Barwala, Distt. Panchkula.
3 Lecturer, Dept of Public Health Dentistry - Swami Devi Dyal Hospital & Dental College, Golpura, Barwala, Distt. Panchkula, India.
4 Professor & H.O.D., Department of Public Health Dentistry, - Swami Devi Dyal Hospital & Dental College, Golpura, Barwala, Distt. Panchkula.
|
| Address For Correspondence |
Dr. Mohit Bansal
Lecturer, Department of Public Health Dentistry
Swami Devi Dyal Hospital & Dental College,
Golpura, Barwala, Distt. Panchkula.
Mobile- 09855701797
Email- mohit.bansal51@gmail.com |
| Abstract |
| Objective: To assess the status of third molar eruption among students of Swami Devi Dyal group of Professional Institutions, Barwala, Panchkula.
Materials and method: A cross-sectional survey was carried out among 969 students aged 18-24 years. Random sampling was done to select the sample size. The eruption status of third molars was recorded on a structured format.
Results: 47.2% (458) were males and 52.7% (511) were females. Females (55.9%) had more number of erupted third molars than males (44.01%).
Conclusion: The number of erupted third molars gradually increased and then decreased with increase in age. The number of extractions of molars also increased with increase in age. |
|
| Keywords |
| molar eruption, phenomenon, eruption, pericoronitis, pathology |
|
| Full Text |
Introduction
Third molars or wisdom teeth are the teeth which are located the furthest back in the mouth. They are usually the last adult teeth to develop and erupt [1]. The literature shows that tooth impaction is a frequent phenomenon [2]. However, there is considerable variation in the eruption status of these teeth in different regions of the jaw [3]. Factors affecting the status of third molar include the selected age group, timing of dental eruption and the radiographic criteria for dental development and eruption [4].
Human jaws are slowly becoming smaller as we cease to chew foods with the vigor and force of our ancestors. If untreated can cause pericoronitis, cellulitis, abscess formation; or untreatable periapical pathology, caries and periodontal disease due to the position of the third molar and its association with the second molar tooth [5]. The third molar, being the last tooth to erupt in the arch, frequently finds itself with insufficient room and so ends up impacted against the distal aspect of the second molar [6].The third molar or wisdom tooth is a frequent source of distress to patients. Thus, the removal of third molars is advised. Many investigators have questioned the necessity of removal of third molar [7]. According to Slaughter' "scientific evidence presented by experts is overwhelmingly in support of the position that the early and expert removal of the malposed, impacted, pathologic or potentially pathologic embedded tooth is the physiologically sound preventive procedure, which is the standard of care practised by all conscientious dental practitioners" [6].
Hence, the present study was undertaken to assess the status of third molar eruption among students of Swami Devi Dyal group of professional Institutions, Barwala, Panchkula.
Materials And Method
Data Collection
A cross-sectional survey was carried out among the students aged 18-24 years of Swami Devi Dyal group of professional Institutions. Simple random sampling was done to select the sample size. The study was conducted during the college hours. Permission for the examination was taken from the respective principals of the colleges. The examination was carried out in the classrooms itself. The minimum age for inclusion was 18 years, because the third molars normally start to erupt by that age. The students above the age group of 24 years and who refused to participate in the study were excluded from the study. All the students were screened by calibrated examiners. Eruption status of third molars was recorded on a structured format using the following criteria.
Erupted (E) - Fully erupted tooth crown at the level of occlusal plane observed in the oral cavity or only one cusp of the tooth crown visible.
Not Erupted (NE) - Tooth was not visible in the oral cavity.
Statistical Analysis
The data's were analyzed using SPSS version 13.0. Chi square analysis was used to find the significance of the cross-tabulation of counts of two or more variables. Student t-test (Unpaired) and analysis of variance (ANOVA) were used to find the significance of the cross-tabulation of a variable with the mean of another variable.
Results
Out of a total of 1045 students, 76
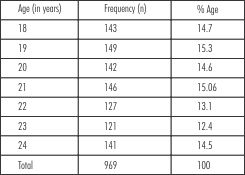 | Table-1 Distribution Of Subjects According To Age
 |
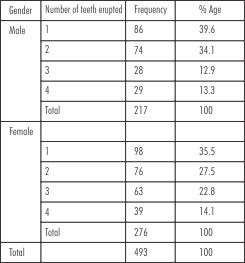 | Table-2 Distribution of erupted teeth according to gender
|
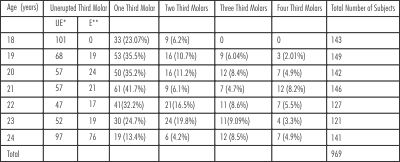 | Table-3 Distribution of erupted teeth according to age
|
students refused to participate in the study. The remaining 969 students were examined with a minimum age of 18 years and a maximum of 24 years. Mean age of the student was 20.9 years. 47.2% (458) were males and 52.7% (511) were females. [Table-1] shows distribution of subjects according to age. The total number third molar teeth erupted and distribution among the students based on sex is described in [Table-2]. The number and distribution of erupted teeth according to the age is presented in [Table-3].
Distribution Of Erupted Teeth According To Age
At the age of 18 years, a total of 143 (14.7%) students were examined. A total of 57 third molars were found to be erupted. Out of 143 students 101 (70.6%) had no third molar (Unerupted teeth) and 33 (23.07%) had only one tooth erupted while 9 (6.2%) had two teeth erupted. None of the subjects were found to have three and all the third molar impacted teeth.
149 students were examined at the age group of 19 years. A total of 77 third molars were found to be erupted. Out of a total of 149 students 68 (37.5%) had no third molar, out of which 19 got extracted (12 of them had got their third molar extracted due to caries and remaining due to pathological reasons as advised by the dentist), 53 (35.5%) had only one erupted third molar, 16 (10.7%) had two teeth, 9 (6.04%) subjects had three teeth erupted while 3 (2.01%) had all the third molars erupted.
At age 20, a total of 142 subjects were examined. A total of 146 third molars were found to be erupted. 57 (40.1%) had no third molars, out of which 24 got extracted (8 of them had got their third molar extracted due to caries and remaining 16 due to pain with respect to second molar). 50 (35.2%) had only one third molar erupted, 16 (11.2%) had two third molars; 12 (8.4%) had three teeth while 7 (4.9%) subjects had all the third molars erupted.
At age group of 21 years, a total of 146 subjects were examined. 57 (39.04%) had no third molars of whom 21 got their molar extracted mainly due to pain as their common complaint and 8 due to caries. 61 (41.7%) had only one third molar, 9 (6.1%) had two third molars, 7 (4.7%) had three third molars; and 12 (8.2%) subjects had all the four third molars erupted in the oral cavity. A total of 148 third molars were found to be erupted.
A total of 127 subjects were examined at the age of 22 years, 47 (37%) had no third molars, of which 2 got extracted due to caries and 11 got their teeth extracted mainly due to pain and 6 got extracted due to pathological reason. 41(32.2%) had one third molar, 21(16.5%) had two molars erupted, 11 (8.6%) had three third molars and 7 (5.5%) had all four third molars erupted. The total number of 144 erupted third molars was present.
At age 23, a total of 121 subjects were examined. 52 (42.9%) had no third molars of which 19 of which got their tooth extracted due to caries and 8 due to pathological reason. 30 (24.7%) had only one third molar erupted; 24 (19.8%) had two third molars; 11(9.09%) had three third molars; and 4 (3.3%) had all four teeth erupted. The total number of 127 impacted third molars was present.
At total of 141 subjects were examined in age group of 24 years. A total of 95 third molars were found to be erupted. 97 (68.7%) had no third molars, out of which 76 had got their third molar extracted mainly due to pathological reasons. 19 (13.4%) had only one third molar; 6 (4.2%) had two third molars; 12 (8.5%) had three third molars; and 7 (4.9%) had all four third molars erupted.
A majority of them got their teeth extracted due to pathological reasons (9.6%) mainly due to pressure causing pain and discomfort resulting in third molar extraction. A few of them got extracted due to presence of caries (6.2%).
Discussion
There is not much information in the literature about the natural history of third molars in young people. The prevalence of one or more third molars in young adults range from 85% to 92% but most have not yet erupted by the time a person is 20 years old. The number of impacted teeth also increased with increase in age. This could be due to the fact that with increase in age and tooth jaw size discrepancy, the tooth is unable to occupy the space in the oral cavity resulting in impaction.
With respect to the surgical removal of third molars, the number of extracted third molars was greater in those who were older, and this was most evident for mandibular molars. In our study 16.1% of 20 years old and 53.9% had one or more third molars extracted which was found to be similar as reported by Hugoson and Kugelber (1988) [8] in which 23% of 20 year olds and 68.3% of 30 year olds had had one or more third molars extracted, whereas Peltola et al (2006) [9] reported that 16.2% of a group of 19-26 year olds had had one or more third molars extracted.
As on today, the fear to visit a dentist is still prevailing in the minds of people. It becomes sometimes difficult for the clinician to convince the patients. In our study 76 subjects refused to participate due to apprehension.
Hence further studies are required to evaluate the actual etiology behind this problem.
Conclusion
Impaction is a frequently encountered clinical problem for the dental surgeon. The main reason behind this is our dietary pattern which has resulted in jaw size discrepancy. Therefore detailed history and evaluation of the condition helps the dentist in planning suitable treatment.
Aknowledgement
The authors thank all the subjects who participated in this study for their co-operation. The authors report no conflict of interest.
References
1. Fields T. Understanding Wisdom Teeth. 1-31.
2. Spencer AJ, Szuster FSP, Brennan DS. Present and future patterns of practice and workforce needs in oral and maxillofacial surgery. Aust Dent J 1992; 37: 222-8.
3. Spencer AJ, Brennan DS, Szuster FSP, et al. Service - mix of oral and maxillofacial surgeons in Australia and New Zealand. Int J Oral Maxillofac Surg 1993; 22: 310-3.
4. Celikoglu M, Miloglu O, Kazanci F. Frequency of agenesis, impaction, angulation, and related pathologic changes of third molar teeth in orthodontic patients. J Oral Maxillofac Surg 2010; 68: 990-5.
5. Management of Unerupted and Impacted Third Molar Teeth A National Clinical Guideline. Scottish Intercollegiate Guideline Network, Number 43. Sign Publications; 1999.
6. John E. Speck. The Widsom Tooth. Can Fam Physician 1981; 27: 664-70.
7. Boboc A, Dibbets J. Prediction of the mesiodistal width of unerupted permanent canines and premolars: a statistical approach. Am J Orthod Dentofacial Orthop 2010; 137: 503-7.
8. Hugoson A, Kugelberg CF. The prevalence of third molars in a Swedish population. An epidemiological study. Community Dent Health 1988; 5: 121-38.
9. Peltola JS, Venta I, Haahtela S, Lakoma A, Ylipaavalniemi P, Turtola L. Dental and oral radiographic findings in first-year university students in 1982 and 2002 in Helsinki, Finland. Acta Odontol Scand 2006; 64: 42-6. |
|
|
|
|
|
|