Introduction:
One of the principal objectives of nonsurgical root canal therapy is to seal the canal system from apical and coronal leakage after cleaning the canal system. Preparation of an apical seat or stop during root canal instrumentation is critical to achieve an apical seal. If an apical stop cannot be developed, it is difficult to prevent extrusion of filling material from the confines of the root canal space during obturation. Such situations are encountered in cases of apical root resorption, apical perforations and immature teeth. These cases require special attention and treatment and it is critical that either a stop be developed or an apical barrier be placed to limit extrusion of obturation material.
Previous investigations have focused on the management of teeth with open apices with calcium hydroxide to develop a calcific bridge that requires patient compliance and multiple appointments.[1] An alternative approach is the placement of an apical barrier to prevent extrusion of root filling materials.
Mineral trioxide aggregate (MTA) was introduced to dentistry in 1993 as a root-end filling material. It has been advocated for use as an apical barrier, repairing perforations, pulp capping and root end induction.[2],[3] This material holds promise because of its sealing capabilities, ability to set in the presence of blood and moisture, and biocompatibility.[4], [5], [6] MTA was originally marketed as a gray coloured preparation. A MTA has later been introduced to provide a hue that matched more closely to that of the colour of the teeth with the elimination of tetracalcium aluminoferrite.
Sluyk SR, Moon PC, Hartwell GR demonstrated that perforation defects repaired with MTA showed that periradicular moisture was advantageous in adapting the material to the walls of the perforation. Further its retention characteristics were not altered by placement of either a moist or dry cotton pellet over the material.[7] Thus, it is reasonable to question whether a moist cotton pellet is needed over the MTA when used as an apical barrier. With an open apex, MTA may set in the presence of periapical moisture; and if this is true, the material could be used in a one-visit procedure.
To date there is limited research comparing the gray coloured and white coloured MTA as an apical barrier material when placed in orthograde manner, with only few case reports showing successful apexification when MTA has been used in two-step procedure. [3], [8].
Hence the purpose of this study was to compare the sealing ability of gray and white MTA, as an apical barrier when placed in orthograde method using one - step or two - step procedure.
Subjects and Methods:
Eighty freshly extracted, single rooted human maxillary anteriors were used in this study. The inclusion criteria for the teeth were as follows: teeth exhibited one canal, which was confirmed by radiographs; had mature apices, no cracks on inspection with operating microscope at 6x magnification, the roots were free from resorption, caries, and restorations, and were not dilacerated.
Specimen Preparation:
The teeth were marked at a level 15mm from the root apex using a measuring ruler. The teeth were then decoronated with a diamond disk to get a standardized 15mm tooth length. To simulate clinical situation of an open apex, the canals were instrumented with Gates Glidden burs #5 - #1 (Mani, Inc. Japan) in a crown down manner until #1 size Gates Glidden bur could pass through the apical foramen. The specimens were then prepared with K-files (Mani, Inc. Japan) until an ISO size 90 file could be visualized 1mm past the apex. Irrigation with 5ml of 3% sodium hypochlorite was used throughout instrumentation and was followed by a final 5ml flush of saline. Teeth were randomly placed into 8 groups of 10 samples each.
To provide a simulated periapical environment, the teeth were mounted onto plastic tubes containing saline soaked Oasis, as previously described by Lee et al.[9] Gray and white MTA (Angelus, Dental Solution, Brazil, Lot No. 9685,3996,2344) were used as apical barrier. The materials were mixed according to manufacturer's instructions and delivered in orthograde manner to the canal space using MTA Carrier (Dentsply, Maillefer, Switzerland) and compacted with prefit hand pluggers.
The experimental groups were divided as follows:
Group 1- 2mm Gray MTA barriers and obturated immediately
Group 2- 2mm Gray MTA barriers and obturated after 24hrs
Group 3- 5mm Gray MTA barriers and obturated immediately
Group 4- 5mm Gray MTA barriers and obturated after 24hrs
Group 5 to Group 8 were identical to Group 1 through Group 4 but white MTA was substituted for gray material.
After the compaction of apical MTA barrier, samples were obturated in following manner.
In Group 1,3,5 and 7 - (immediate obturation)
The samples were obturated immediately with AH - Plus sealer (Dentsply, De Trey, Germany, Lot No.60620112) and thermoplasticised gutta-percha using the Obtura II (Obtura Spartan, Fenton, MO)
Group 2,4,6 and 8 (Obturation After 24 hours)
A moist cotton pellet was placed over the MTA and the access cavities were sealed with Cavit G (3M ESPE AG, Germany). MTA was allowed to set at 37°C and 100% humidity for 24 hours and then the remaining canal space was obturated in similar manner as in the one step group.
The coronal portion of all samples were sealed with glass ionomer cement and stored in saline soaked Oasis for 1 week at 37°C. After one week, the samples were removed and double coated with nail varnish except for the apical 2mm. The teeth from all groups were placed in Methylene blue dye for 48 hours. To determine the depth of dye penetration, each specimen was sectioned longitudinally with slow speed diamond saw.
All sections were evaluated under an operating microscope (Carl Zeiss, Germany) at 6x magnification and digital images were captured and saved as TIFF image. The images were given random numbers by a person not evaluating the samples. This is for the evaluator to be blinded to the samples being measured. One evaluator measured the amount of apical dye migration using measuring ruler in Adobe Photoshop version 7.0. The image numbers were then decoded back to their original group.
This linear dye measurement was then converted to a percentage of dye penetration through the entire length of the barrier. A one-way ANOVA was used to determine the statistical difference regarding type of MTA, technique, and barrier thickness.
Results:
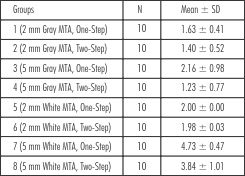
In the present study, type of MTA, one or two step technique and the thickness of the barrier yielded significant results. Gray MTA (P<0.001; Table 1) demonstrated significantly less dye leakage as compared to white MTA (P<0.001; Table 2). Six out of forty gray MTA barriers showed complete dye penetration after 48 hrs whereas 28 out of 40 samples of white MTA revealed complete dye penetration through the barrier. The mean leakage values and the mean percentage leakage values of gray and white M.T.A. are given in Table 4 and 5 respectively. The two step technique demonstrated significantly less leakage than the one step technique of barrier placement (P<0.001; Table 5; Fig 1). The 5mm MTA barrier also performed significantly better than the 2mm barrier (P< 0.001; Table 6; Fig 2).
 | Table 1 Extent of Linear Dye Penetration in Gray MTA Apical Barrier (in mm)
 |
 | Table 2 Extent of Linear Dye Penetration In White MTA Apical Barrier (in mm)
|
Discussion:
Cessation of root development caused by trauma, caries or other pulpal pathosis requires special treatment. The apical architecture makes complete debridement and control of the obturation material very difficult. Moreover, these roots are often thinner and therefore more brittle.[10]
Despite its popularity for apexification procedure, calcium hydroxide therapy has some inherent disadvantages, including variability of treatment time, unpredictability of apical closure, difficulty in patient follow up, and delayed treatment.[11] Therefore the search continues for procedures and materials that may allow for more natural continued apical closure in teeth with immature apices in shorter duration of time.Mineral Trioxide Aggregate (MTA) is a powder that consists of fine hydrophilic
 | Table 3 Mean Leakage Values (mm) of Gray & White MTA
|
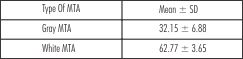 | Table 4 Mean % Leakage Values of Gray & White MTA
|
[ 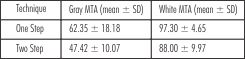 | Table 5 Mean % Leakage Values of Gray & White MTA in One-Step & Two-Step Techniques
|
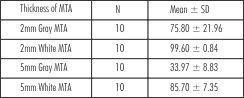 | Table 6 Mean % Leakage Values of Gray & White MTA at 2mm & 5mm Barrier thickness
|
particles that in the presence of moisture forms colloidal gel that solidifies to form hard cement within 4 hours. MTA was originally marketed as a gray coloured preparation and has been associated with occasional staining of the teeth. Therefore, a white MTA material has been developed to overcome this concern. The principal components of gray MTA are tricalcium silicate, dicalcium silicate, tricalcium aluminate, tetracalcium aluminoferrite and calcium sulfate dihydrate. In addition to these components mineral oxides have been added that are responsible for chemical and physical properties of this aggregate.[9] Tetracalcium aluminoferrite is reportedly removed in the white formulation so as to provide a hue that matched more closely to that of the teeth.[12]
The manufacturer's recommendation for mixing has been stringently followed to avoid decreasing the optimum properties of the material. In the present study, MTA was placed into the canal using hand condensation. Research has shown that hand condensation showed better adaptation to the tube walls than ultrasonic method. [13] Aminoshariae A et
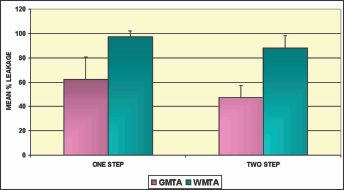 | Fig 1 - Leakage Results: One-Step versus Two-step Techniques (P < 0.001)
|
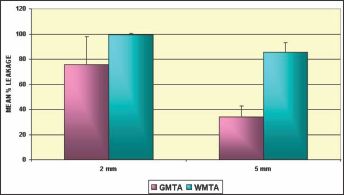 | Fig 2 - Leakage Results: 2mm versus 5mm Barrier Thickness (P < 0.001)
|
al also revealed that the manufacturer's recommended water-to-powder ratio is not favorable for ultrasonic condensation for the placement of MTA. [13]
The idea of single visit apexification is not new and has been discussed and tested for many years.[14],[15] The success rate varies for different materials. A material like MTA with a high biocompatibility is a viable option, but still needs further testing. This material is osteoconductive [11], which may help the periapical tissue to adapt and heal.
Although one-step apexification procedures with MTA have been advocated by Giuliani V et al. [16], Maroto M et al. [8], Kratchman SI[10], it has been shown by Matt G et al.[17] and Sarkar NK et al.[18] that additional moisture from a cotton pellet is crucial for the material to establish its optimum properties. These findings concur with the manufacturer's recommendation of placing a moist cotton pellet in the canal, temporizing and allowing the material to set for a minimum of 4 hrs. Hence it was decided in this study to investigate the sealing ability of both one-step (immediate obturation) and two-step (obturation after 24hrs) technique.
The manufacturer of MTA recommends a 3mm to 5mm thickness of MTA for apexification procedure. We chose to investigate the sealing ability of the material at 2mm because this would be the minimum depth of MTA required with gutta-percha obturation to simulate a clinical situation[19] and at 5mm since clinically a barrier of 5mm (within manufacturer's recommended guidelines) may be considered if root end surgery is a treatment option. Evidence have shown that teeth obturated with orthograde MTA and followed by root-end resection showed periradicular healing similar to teeth with fresh MTA placed as root end filling material.[20] If a 3mm root end resection had to be performed after placement of 5mm MTA apical barrier, then no root end filling would have to be placed at the time of surgery.
In the present study 5mm of gray MTA barrier, in a two-step technique demonstrated significantly less dye leakage than white MTA (P < 0.001).The results of this study are in agreement with those of Matt G et al.[17] The manufacturer recommends the canals be medicated with calcium hydroxide for one week, prior to MTA treatment. The rationale is to enhance the debridement of the canal. We do not know whether or not this has an effect on the sealibility of MTA, because we did not use calcium hydroxide in this study. A previous study by Hachmeister et al showed that the calcium hydroxide has no effect on the sealability of MTA.[21]
We believe that it is important to evaluate the sealing ability of an MTA apical barrier condensed into root-end preparation as orthograde delivery is very technique sensitive. Placement must be verified with radiographs and condensation is limited because of minimal resistance of the open apex. In addition to the difficulty in delivering the material to the apex, the irregularity and divergent nature of the anatomy may limit adaptation to the dentinal walls, creating marginal gaps at the dentinal interface.
In the present study gray MTA, demonstrated significantly less dye leakage as compared to white MTA. The reason for this could be the significant reduction of tetracalcium aluminoferrite from the white MTA.[12] This might alter the properties of white MTA such as slight volumetric shrinkage which could have accounted for the increased leakage seen with this material.
The two-step technique performed better than the one-step technique. The reason could be that MTA powder consists of fine, hydrophilic particle that set in the presence of moisture. The setting reaction of MTA has been explained by Sarkar NK et al.[18] Though it is possible that moisture from the periapical environment may be sufficient for MTA to set, it has been shown clearly that additional moisture from the cotton pellet is crucial for MTA to establish its optimum properties. [17]
The 5mm barrier also performed significantly better than the 2mm barrier because they could be condensed more thoroughly since the placement would have become much easier due to increased resistance to dislodgment through the open apex as observed by Aminoshariae A et al.[13]
Based on the results of this study, the gray MTA has performed significantly better in all the parameters tested. With the advent of MTA, a more efficient and permanent apexification can be performed in a time bound manner showing good sealing ability, good marginal adaptation, high degree of biocompatibility.However further research can be carried out to improve the method of orthograde delivery of apical MTA barrier and behaviour of immature root to MTA.
References:
1. Frank AL. Therapy for the divergent pulpless tooth by continued apical formation. J Am Dent Assoc 1966; 72: 87-93.
2. Schwartz RS, Mauger M, Clement DJ, Walker III WA. Mineral trioxide aggregate: a new material for endodontics. J Am Dent Assoc 1999; 130: 967-975.
3. Torabinejad M , Chivian N. Clinical applications of mineral trioxide aggregate. J Endod 1999; 25: 197 - 205.
4. Keiser K, Johnson CC, Tipton DA. Cytotoxicity of mineral trioxide aggregate using human periodontal ligament fibroblasts. J Endod 2000; 26: 288 - 291.
5. Koh ET, McDonald F, Ford TRP, Torabinejad M. Cellular response to mineral trioxide aggregate. J Endod 1998; 24: 543 - 547.
6. Nakata TT, Bae KS, Baumgartner JC. Perforation repair comparing mineral trioxide aggregate and amalgam using an anaerobic bacterial leakage model. J Endod 1998; 24: 184 - 186.
7. Sluyk SR, Moon PC, Hartwell GR. Evaluation of setting properties and retention characteristics of mineral trioxide aggregate when used as a furcation perforation repair material. J Endod 1998; 24: 768 - 771.
8. Maroto M, Barberia E, Planells P, Vera V. Treatment of non-vital immature incisor with mineral trioxide aggregate. Dent Traumatol 2003; 19: 165 - 169.
9. Lee SJ, Monsef M, Torobinejad M. Sealing ability of mineral trioxide aggregate for repair of lateral root perforations. J Endod 1993; 19: 541 - 544.
10. Kratchman SI. Perforation repair and one-step apexification procedures. Dent Clin N Am 2004; 48: 291- 307.
11. Shabahang S, Torabinejad M, Boyne PP, Abedi H, McMillan P. A comparative study of root end induction using osteogenic protein-1, calcium hydroxide and mineral trioxide aggregate in dogs. J Endod 1999; 25: 1-5.
12. Asgary S, Parirokh M, Eghbal MJ, Brink F. Chemical difference between white and gray mineral trioxide aggregate. J Endod 2005; 31: 101- 113.
13. Aminoshariae A, Hartwell GR, Moon PC. Placement of mineral trioxide aggregate using two different techniques. J Endod 2003; 29: 679- 682.
14. Harbertz H. Generic tricalcium phosphate plugs: an adjunct in endodontics. J Endod 1991; 17: 131 - 134.
15. Rossmeisl R, Reader A, Melfi R, Marquard J. A study of freeze-dried (lyophilized) cortical bone used as an apical barrier in adult monkey teeth. J Endod 1982; 8: 219 - 226.
16. Giuliani V, Baccetti T, Pace R, Pagavino G. The use of MTA in teeth with necrotic pulps and open apices. Dent Traumatol 2002; 18: 217-221.
17. Matt GD, Thorpe JR, Strother JM, McClanahan SB. Comparative study of white and gray mineral trioxide aggregate simulating a one-or two-step apical barrier techniques. J Endod 2004; 30: 876 - 879.
18. Sarkar NK, Caicedo R, Ritwik P, Moiseyeva R, Kawashima I. Physiochemical basis of the biologic properties of mineral trioxide aggregate. J Endod 2005; 31: 97-100.
19. Al-Kahtani A, Shostad S, Schifferte R, Bhambhani S. In vitro evaluation of micro leakage of an orthograde apical plug of mineral trioxide aggregate in permanent teeth with simulated immature apices. J Endod 2005; 31: 117-119.
20. Apaydin ES, Shabahang S, Torabinejad M. Hard tissue healing after application of fresh or set MTA as root-end filling material. J Endod 2004; 30: 21 - 24.
21. Hachmeister DR, Schindler WG, Walker III WA, Thomas DD. The sealing ability and retention characteristics of mineral trioxide aggregate in a model of apexification. J Endod 2002; 28: 386-390. |