Introduction :
The frontal sinus bud is present at birth in the ethmoid region but is not evident radiographically until the fifth year, when it projects above the orbital rim[1]. Rapid growth of the sinus continues until the age of 12 years[2]. Tanner[3] found that the annual height (stature) increments in children reached a plateau at 16 years in boys and 14 years in girls, and it was thought that these, too, were the ages at which frontal sinus enlargement ceased. This suggests that the increase in the sinus size very closely follows a growth trend similar to that of other bones. Joffe[4], Rossouw et al[5] found frontal sinus enlargement to be associated with prognathic subjects.
However, there is lack of anteroposterior and vertical relation classification specificity in these studies, therefore additional data was necessary. The present study was carried out with the following aims and objectives:
1. To assess the area of the frontal sinus in various skeletal malocclusion groups.
2. To compare the area of the frontal sinus in various skeletal malocclusion groups.
3. To correlate the area of frontal sinus with other variables of mandibular growth.
Materials And Methods
The present study was conducted on 80 pre-treatment lateral head cephalograms, obtained from the patient record files, and the patients attending the OPD of the Department of Orthodontics and Dentofacial Orthopaedics, Faculty of Dental Sciences, CSMMU Lucknow. Age of the subjects ranged from 16 to 25 years (mean age 17.76 years), indicating young adult sample.
The sample was divided according to antero-posterior skeletal relationships into skeletal class I, class II and class III malocclusion based upon the ß-angle (Chong Yol Baik and Maria Ververidou[6]) measurement as shown in (Table-1).
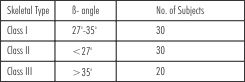 | Table 1
 |
The same sample was also divided according to vertical skeletal relationships into Hypodivergent, Neutral (Normodivergent) and Hyperdivergent on the basis of facial height ratio (FHR), or Jarabak quotient (Siriwat and Jarabak[7]) (Table-2).
 | Table 2
|
The division of the subjects on the basis of sex was not undertaken due to unequal distribution and narrow sample size. There was no history of previous orthodontic treatment or trauma to dentofacial region and TMJ. Individuals with micrognathia, macrognathia and other syndromes of oro-facial region were excluded.
All cephalometric radiographs were traced on an acetate paper of 0.5µ thickness with sharp 4H pencil on a view box. The tracings were done under trans-illuminated light in a dark room. Precautions were taken to eliminate stray light.
In tracing of bilateral anatomic structures, a line midway between right and left sides was used. This allowed the consideration of all structures as being in the midline and also helped to eliminate errors caused by improper positioning of patient during exposure of X-ray film. All the linear measurements were read to the nearest 1mm on a standard millimeter ruler. Degrees were likewise measured to the nearest 1° by a Protractor.
Frontal sinus was calculated by superimposing a transparent standard graph sheet over the tracing of lateral head cephalogram and counting the number of squares within the inner outline of frontal sinus. The cross sectional area was expressed in square millimeters. When more than half area of the square was within the perimeter of frontal sinus, it was also counted as full square, where as squares having less than half of the areas inside the perimeter were excluded from the count.
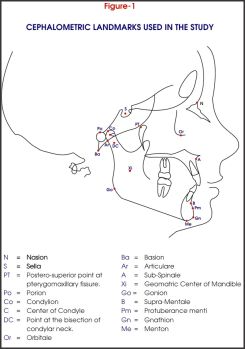
Various variables of abnormal mandibular growth, jaw sizes, positional changes and growth direction were used (Figure 1, 2, 3, & 4).
 |
|
 |
|
 |
|
 |
|
The results of this cross-sectional study were analyzed. Mean values of different variables were calculated within each Class- ClassI, Class II, ClassIII and each Group- Group I (Hypodivergent), Group II (Normodivergent), Group III (Hyperdivergent). Correlation coefficients were used to assess relation between the frontal sinus and the other variables drawn on the lateral cephalometric radiograph, so as to check the reliability of frontal sinus as an indicator of mandibular growth.
Results & Discussion
Malocclusion has been interpreted to be unfavorable deviations from the norms, and their morphologic characteristics have been studied extensively by analysis of the lateral cephalograms.
Some authors have related Frontal Sinus Area to various malocclusions. Acromegaly is associated with prominent frontal sinus and overgrowth of the jawbone, and one usually finds a class III-type prognathic mandible in these cases (Shafer, Hine, Levy, 1974) [8]. Joffe (1964)[4] found Frontal Sinus enlargement to be associated with prognathic subjects, but no indication was given as to the correlation with indicators of growth-prediction.
Rossouw, Lombard, Harris (1991)[5] correlated Frontal Sinus Area with excessive mandibular growth. Ruf and Pancherz(1996) [9],[10] suggested that the somatic maturity stage may be predicted rather accurately by analyzing Frontal Sinus development on pre-existing lateral head cephalograms.
The present study was carried out to analyze the size of Frontal Sinus in different craniofacial patterns and also to assess whether the size of Frontal Sinus could be correlated with mandibular growth. Age range of 16-25 years (mean age 17.76 years) was chosen to get a sample with Frontal Sinus growth completed. Dolan, (1982)[2] reported that the growth of sinuses continues until the age of 12 years, when they reach nearly adult size. Tanner (1962)[3] found that the annual height increments in children reached a plateau at 16 years in boys and 14 years in girls, and it was thought that these, too, were the ages at which Frontal Sinus enlargement ceased. Ruf and Pancherz (1996)[9] reported that Frontal Sinus shows peak growth at an average age of 15.1 years in males. According to Brown, Molleson and Chinn (1984)[11] enlargement of the frontal sinus ceases at 15 ½ years in boys and 13 ¾ years in girls. The division of subjects on the basis of sex was not carried out because of unequal distribution and narrow sample size.
Five measurements proposed by Ricketts (1982)[12] were used to determine the presence of abnormal mandibular growth: Cranial Deflection, Porion Location, Ramus Position, Symphysis Width, Condylar Axis. Schulhof, Nakamura, Williamson (1977)[13] found that a high Cranial Deflection, short Porion Location, forward Ramus Position, and Class III molar relation were telltale signs that excessive mandibular growth was likely to occur. They claimed 73% prediction accuracy with these four factors. Ricketts (1982)[12] claimed that with these four factors along with Symphysis Width and Condylar Axis, accuracy in predicting abnormal mandibular growth increased to approx. 90%. In our study we chose only skeletal criteria, thus class III molar relation was not used as a parameter.
The ANB Angle (Steiner, 1953)[14] is still widely accepted as an indicator of maxillo-mandibular harmony (Jacobson, 1975)[15]. Therefore , it was used to assertain its correlation with the Frontal Sinus Area.
The facial axis angle (Ricketts, 1975)[16] and the FMA (Tweed, 1946)[17] were measured to give an indication of growth direction. Effective Maxillary Length and Effective Mandibular Length (McNamara, 1984)[18] were measured to give an indication of the size of the jaw bones. Saddle Angle and Articular Angle were measured to give an assessment of positioning of the mandibular condyle to the cranial base, to see whether it is the position of condyle, which ultimately affects the mandibular positioning (Rakosi, 1982) [19].
Gonial angle was used as it is an expression for the form of mandible, with reference to the relation between body and ramus. It also gives information of the mandibular growth direction (Rakosi, 1982) [19].
Assessment Of Frontal Sinus Area In Various Skeletal Types, Followed By Inter-class And Inter-group Comparisons
The mean value of the Frontal Sinus Area, as seen on the lateral cephalogram was found to be larger in skeletal Class III (310.50±68.07) malocclusion as compared to skeletal Class I (203.33±66.02) malocclusion. The difference of their means was very highly significant. Similar findings were reported by Joffe (1964)[4], who found Frontal Sinus enlargement to be associated with prognathic subjects. The findings of the present study were also in agreement with those of Rossouw, Lombard and Harris (1991)[5]. They reported a Frontal Sinus mean size of 330.81±199.17 mm[2] and statistically demonstrated that a larger Frontal Sinus Area was associated with excessive mandibular growth, as in case of skeletal Class III malocclusion.
Singh, McNamara and Lozanoff (1997)[20] compared class I and class III cranial base configuration using FEM (Finite Element Analysis) for size change and reported dilations within anterior cranial base. Some earlier studies suggested that increase in thickness in the region of nasion was accounted for by enlargement of the frontal sinus (Bjork, 1955[21], Scott, 1958[22]).
In the present study, on comparison of Frontal Sinus Area in skeletal class II (219.07±62.83) and skeletal Class III (310.50±68.07) malocclusions, the area was found to be larger in skeletal Class III malocclusion. Skeletal class III and class II malocclusion are the extreme variations of the facial developmental process, depicting excessive and deficient mandibular growth respectively, so it was logical to look for a significant difference between the two malocclusions, which was shown by the present study.
Sollow and Nielsen (1992)[23] had suggested that since facial growth types, which deviate from the norm, would be expected to leave the most dramatic traces in the facial structures, the structurally based methods should predict extreme facial development better than the methods based on average increments.
On comparing the Frontal Sinus Area in skeletal class I malocclusion with skeletal class II malocclusion, the results were found to be non-significant. On seeing the significant results of skeletal class I and skeletal class III comparison, one may logically assume that small frontal sinuses should have been associated with small mandibles. But the present study reported no significant difference between the Frontal Sinus Area in skeletal class I and skeletal class II malocclusion.
It showed that though the Frontal Sinus Area increased with mandibular prognathism as in skeletal class III cases, the reverse was not true, that it was not found to decrease in skeletal class II malocclusion as compared to skeletal class I malocclusion. In a similar study reported by Rossouw, Lombard and Harris (1991)[5] they had only compared the area of the frontal sinus in between adult skeletal class III and adult skeletal class I growth pattern cases but did not study the class II growth pattern cases.
In the vertical plane, the Frontal Sinus Area did not vary significantly between Hypodivergent (243.43±79.21) & Normodivergent (221.65±80.74) and Hyperdivergent (221.30±67.80) group. The non- significance of the Frontal Sinus Area in these groups might be due to the fact that all skeletal classes i.e. skeletal Class I, II, and III malocclusions were distributed in the Hypodivergent, Normodivergent and Hyperdivergent groups.
Assessment Of Correlation Of Frontal Sinus Area With Various Variables Of Mandibular Growth In Skeletal Class I, Class Ii And Class Iii Malocclusions
Karl Pearson's correlation coefficients were calculated between Frontal Sinus Area and other variables in skeletal Class I, II and III malocclusions. Correlation coefficients were not calculated in Group I, II and III, as there was no significant difference of the Frontal Sinus Area in these groups.
Correlation with ß -angle & ANB:
A large ß angle is indicative of a large mandible and a small maxilla as expressed in skeletal Class III malocclusion. Reverse is true for skeletal Class II malocclusion.
The positive correlations between Frontal Sinus Area and ß angle were not significant for this sample but confirmed the mandible and the Frontal Sinus association. (i.e. a large angle goes with a large frontal sinus). Similarly, negative correlation between the Frontal Sinus and ANB angle was not significant for the sample but confirmed the mandible and the Frontal Sinus association.
Correlation with Facial Axis Angle, FMA, Facial Height Ratio & Gonial angle:
The poor correlation suggested that large Frontal Sinus may be present with large mandible irrespective of its growth direction, or the form of mandible, with reference to the relation between body and ramus.
Correlation with Saddle Angle & Articular Angle:
Saddle Angle indicates the relationship between anterior and posterior-lateral cranial bases. It signifies the position of the condyle with that of cranial base. Articular Angle also signifies the position of the condyle.
The poor correlative results of the present study suggested that large frontal sinus was associated with large mandible irrespective of its relation to the cranial base.
Correlation with Cranial Deflection:
In case of skeletal Class III malocclusion, in the present study, there was a positive correlation between Cranial Deflection and Frontal Sinus Area (r = 0.47) and the value was statistically significant.
The results showed that a large Frontal Sinus Area was associated with a large Cranial Deflection in skeletal Class III malocclusion. Schulhof, Nakamura and Williamson (1977)[13] in their study on Class III malocclusion have reported that large Cranial Deflection is associated with prognathic mandibles. This is mainly due to descend of the posterior cranial base resulting in the anterior positioning of the mandible.
Correlation with Porion Location:
Correlations between Porion Location and Frontal Sinus Area were found to be low and non-significant Schulhof, Nakamura and Williamson (1977)[13] concluded that short Porion Location is suggestive of excessive mandible growth. However, short Porion Location is basically due to anterior positioning of mandible relative to maxilla and cranial base.
The results of present study showed that large Frontal Sinus Area was associated with large mandible irrespective of its positional relationship to maxilla and/or cranial base. The present study findings were similar to the findings reported by Rossouw, Lombard and Williamson (1991)[5] in which they reported a non-significant correlation between porion location and Frontal Sinus Area
Correlation with Condylar Length:
The positive correlation value of Condylar Length with Frontal Sinus Area suggested that large Frontal Sinus Area was associated with large Condylar Length, which was associated with mandibular prognathism (Ricketts, 1982) [12].
Rossouw, Lombard and Harris(1991)[5], had also reported a positive correlative coefficient (r = 0.233), which was significant (p<0.05), for the sample consisting of skeletal Class I and Class III cases. The non-significant values in the present study may be due to smaller sample size.
Correlation with Symphysis Width:
In the present study there were positive correlations between Symphysis Width and Frontal Sinus Area in skeletal Class I and Class III malocclusion, the values being non-significant, though it was clinically important in the later. In case of skeletal Class II malocclusion very highly significant positive correlation was found.
These findings suggested that large Frontal Sinus Area was associated with large mandible with large symphysis width. Ricketts (1982)[12] reported that large symphysis width was associated with large mandibles. Todd, Aki and Nanda (1994)[24] assessed the symphyseal dimensions as a predictor of the direction of mandibular growth.
The present study findings were similar to those, reported by Rossouw, Lombard and Harris (1991)[5], who also reported positive correlation between Symphysis Width and Frontal Sinus Area. Non-significance of the correlation value in skeletal Class III malocclusion in the present study may be due to small sample size.
Correlation with Effective Maxillary Length/Mandibular Length:
There were positive correlations with Frontal Sinus Area in skeletal Class I and Class III malocclusion. In case of skeletal Class II malocclusion significant correlation was found.
Guyer, Ellis and McNamara (1986)[25] have reported larger mandibular length in skeletal class III sample as compared to skeletal class I sample. The results of present study suggested association between large mandible and Frontal Sinus Area. The non-significance of the correlation coefficient in skeletal Class I and Class III malocclusion may be due to insufficient sample size.
To adequately analyze Fontal Sinus size, an occipitomental radiograph may also be used (Harris, Wood, Nortje and Thomas)[26], but that was beyond the purpose of this study. The lateral cephalogam is part and parcel of everyday orthodontic analyses, and this study indicates that a large frontal sinus as seen on the lateral cephalograms may give an indication to excessive mandibular growth.
Although this method seems to be promising, there are some inherent limitations in its present form. The frontal sinus is exposed to muscle attachments and to influences from the external environment that play a part in its size (Rossouw, Lombard and Harris ,1991)[5]. Body stature may also be associated with Frontal Sinus Area, as seen in cases of acromegaly (Shafer, Hine and Levy,1974)[8]. Being a cross-sectional study a clear cut relation between the Frontal Sinus Area and mandibular growth could not be drawn. Probably the limitations of the study can be minimized by doing the study on a large sample size and undertaking an elaborate longitudinal study.
Conclusion
Foregoing the observations, the following conclusions were drawn:
1. Frontal Sinus Area, as seen on a lateral cephalogram, tends to be larger in individuals having skeletal Class III malocclusion as compared to skeletal Class I and Class II malocclusions.
2. There are no significant variations in the Frontal Sinus Area in individuals with Hypodivergent, Normodivergent and Hyperdivergent facial forms.
3. Large Frontal Sinuses are associated with large mandibles, irrespective of their positional relationship to the cranial base and growth direction.
References
1. Harris AM, Wood RE, Nortjé CJ, Thomas CJ. Gender and ethnic differences of the radiographic image of the frontal region. J Forensic Odontostomatol 1987;5:51-7.
2. Dolan KD. Paranasal sinus radiology. Part IA. Introduction and the frontal sinuses. Head Neck 1982;4:301-11.
3. Tanner JM. Growth at adolescence. 2nd ed. Oxford: Blackwell Scientific Publications, 1962;3.
4. Joffe BM. Frontal sinus enlargement associated with mandibular prognathism. J Dent Assoc S Afr 1964:127-9.
5. Rossouw PE, Lombard CJ, Harris AMP. The frontal sinus and mandibular growth prediction. Am J Orthod Dentofac Orthop 1991;100:542-6.
6. Chong Yol Baik, Maria Ververidou. A new approach of assessing sagittal discrepancies: The Beta angle. Am J Orthod Dentofac Orthop 2004;126:100-5.
7. Siriwat PP, Jarabak JR. Malocclusion and Facial Morphology Is there a Relationship? An Epidemiologic Study. Angle Orthod 1985;55(2):127-138.
8. Shafer WG, Hine MK, Levy BM. A textbook of oral pathology. 3rd ed. Philadelphia: WB Saunders, 1974:606-7.
9. Ruf S, Pancherz H. Development of the frontal sinus in relation to somatic and skeletal maturity. A cephalometric roentgenographic study at puberty. Eur J Orthod 1996; 18(5):491-97.
10. Ruf S, Pancherz H. Frontal sinus development as an indicator for somatic maturity at puberty? Am J Orthod Dentofac Orthop 1996; 110:476-82.
11. Brown WAB, Molleson TI, Chinn S. Enlargement of the frontal sinus. Ann Hum Biol 1984;11:221-6.
12. Ricketts RM, Roth RH, Chaconas SJ, Schulhof RJ, Engel GA. Orthodontic diagnosis and planning. No. 1. Denver, Colorado: Rocky Mountain/Orthodontics, 1982;28:243-60.
13. Schulhof RJ, Nakamura S, Williamson WV. Prediction of abnormal growth in Class III malocclusions. Am J Orthod 1977;71:421-30.
14. Steiner CC. Cephalometrics for you and me. Am J Orthod 1953;39:729-55.
15. Jacobson A. The "Wits" appraisal of jaw disharmony. Am J Orthod 1975;67:125-38.
16. Ricketts RM. A four-step method to distinguish orthodontic changes from natural growth. J Clin Orthod 1975;9:208-28.
17. Tweed CH. The Frankfort-mandibular plane angle in orthodontic diagnosis, classification, treatment planning, and prognosis. Am J Orthod 1946,32,175-230.
18. McNamara JA, Jr. A method of cephalometric evaluation. Am J Orthod 1984;86:449-69.
19. Thomas Rakosi. An atlas and manual of cephalometric radiography. Wolfe Medical Publications Ltd, 1982.
20. Singh GD, McNamara JA, Lozanoff S. Finite Element Analysis of the Cranial Base in Subjects with Class III Malocclusion. Br J Ortho1997;24:103-112.
21. Björk A. Cranial base development. Am J Orthod 1955, 41, 198-255.
22. Scott, J. H. The cranial base. Am J Phys Anthropology 1958, 16, 319-348.
23. Solow B, Siersbæk-Nielsen S. Cervical and craniocervical posture as predictors of craniofacial growth. Am J Orthod Dentofac Orthop 1992;101:449-58.
24. Aki T, Nanda RS, Currier GF, Nanda SK. Assessment of symphysis morphology as a predictor of the direction of mandibular growth. Am J Orthod Dentofac Orthop 1994;106:60-9.
25. Guyer EC, Ellis EE, McNamara JA, Behrents RG. Components of Class III malocclusion in juveniles and adolescents. Angle Orthod 1986;56:7-30.
26. Harris AM, Wood RE, Nortjé CJ, Thomas CJ. The frontal sinus: forensic fingerprints? A pilot study. J forensic Odontostomatol 1987;5:9-15. |