Introduction
Odontogenic tumors constitute a group of heterogeneous lesions that range from hamartomatous or non neoplastic tissue proliferation to malignant neoplasm with metastatic capacity. They may originate from the epithelial and / or ectomesenchymal odontogenic tissues, exhibiting varying degree of intertissue interaction. Adenomatoid odontogenic tumor (AOT) is a benign odontogenic jaw lesion arising from enamel organ or dental lamina.
A marked geographic variation is apparent in the relative incidences of Adenomatoid odontogenic tumor (AOT) in English literature and our review. It is more prevalent in Asian and American populations than in European and African populations[1]. This indicates differences in their distribution from one geographic region to another. Only limited published series on odontogenic tumors are available from other countries (China [2], [3], Hongkong [4], Malaysia [5],[6], Srilanka [7]).
A retrospective study of Adenomatoid odontogenic tumor (AOT) was undertaken and these cases had been analyzed according to age, sex, location, duration of lesion, signs & symptoms, radiographic findings, histopathological appearances and various treatment modalities used. An attempt was made to correlate these findings with the studies carried out in the past in different countries and to update the biological profile of Adenomatoid odontogenic tumor (AOT).
Materials & Methods
197 cases of odontogenic tumors were retrieved from the files of Department of Oral Pathology & Microbiology, Govt. Dental College & Hospital, Nagpur in the period of 1978 to 2003. Out of them, in accordance with the WHO classification of odontogenic tumours, 30 cases were found to be of Adenomatoid odontogenic tumor (AOT). After seeking permission from the institutional ethical committee, the Adenomatoid odontogenic tumor (AOT) was reviewed considering parameters like age, sex, location, duration, radiographic findings, histopathological appearances and treatment modalities. The results were further compared with the studies conducted in other parts of the world. Statistically, p< 0.05 was considered to be significant.
Observations And Results
Frequency: 30 cases of Adenomatoid odontogenic tumor (AOT) were found in this review, accounting for 15.1% of odontogenic tumors. According to this review, it ranks second in comparison to other studies where it ranks fourth or fifth among 'top ten' of odontogenic tumors.
Age: In this review, AOT most commonly occurred in the second and third decades with 19 cases in the 10-19 yrs and 10 cases in the 20-29 yrs. The mean age of occurrence of AOT was 18.7 yrs.
Gender: Among the 30 cases of AOT, there were 10 males and 20 females with male: female ratio of 1: 2.
 | Table 1 Gender Distribution By Age Groups In Adenomatold Odontogenic Tumor (ADT)
 |
From the cross tabulation shown above, there were 5 males and 14 females with M:F ratio 0.36:1 in the second decade as compared to M:F ratio of 1:1 in the third decade. Only a single female was reported in 30 and older age groups.
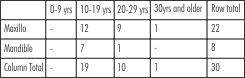 | Table 2 Location Of AOT By Age Groups
|
When the distribution of cases between maxilla and mandible was further analyzed according to age groups, it is seen that the maxilla is the predilection site in second and third decades while mandible is most commonly involved in second decade.
 | Table 3 Location of AOT by Gender
|
Out of 22 cases of maxilla, 8 were male and 14 were female (male: female ratio0.57:1) while in 8 cases of mandible, 2 were male and 6 were female (male: female 1: 3).
The majority of AOT lesions were of the intrabony type. Out of 30 cases, 29 cases of intrabony type (96.7%) were reported of which the follicular AOT accounted for 19 cases (65.5%) and the extrafollicular AOT accounted for 10 cases (34.5%) and one case of peripheral AOT was reported (3.3%). Hence, the follicular variant was 1.9 times as frequent as the extrafollicular variant.
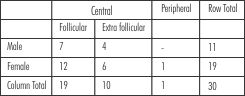 | Table 4 Distribution of AOT variants by Gender
|
The follicular type showed a M:F ratio of 0.58:1, the corresponding Figures for extrafollicular type are 0.67.
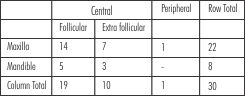 | Table 5 Distribution of AOT variants by Location
|
The follicular variant shows maxilla: mandible ratio of 2.8:1, the corresponding figures for extrafollicular type are 2.3:1. A single case of peripheral AOT was reported in the maxilla of a 17 yrs old female.
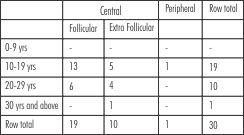 | Table 6 Distribution of AOT variants By Age Groups
|
This indicated that the follicular type was diagnosed at an earlier age than the extrafollicular type. This is certainly due to the fact that follicular AOT is associated with embedded tooth, leading to its eruption failure. Hence, raising the concern of the patient to seek dental advice, resulting in early diagnosis.
Out of 19 cases of follicular AOT, 13 were associated with one tooth and 6 were associated with 2 or more teeth. The most common embedded tooth noticed was permanent canine (13 cases, 68.4%) and upper canine alone in 10 cases (52.6%).
Radiographically, it reveals a destructive lesion of the jaw which may or may not be well circumscribed except in follicular AOT, where it resembles a dentigerous cyst. The lesions are almost invariably unilocular radiolucenies but may contain faint to dense radiopaque foci. Separation of roots or displacement of adjacent teeth occurs frequently but root resorption is rare.
Histopathological features: The AOT is made up of epithelial cells, usually with scanty connective tissue. These polyhedral or spindle shaped epithelial cells vary in their pattern from nests, sworls or cords to cells of a definite columnar or cuboidal variety arranged in duct like pattern. The lumina of these duct like structures contain an eosinophilic coagulum. Droplets of eosinophilic material are found are frequently found between epithelial cells arranged in solid patterns. Foci of calcification are scattered through out the tumor and is interpreted as attempted enamel formation. Fig 1 & 2
Treatment and recurrence; Conservative surgical enucleation was done in all 24 cases without any recurrences, 6 patients did not come for the treatment.
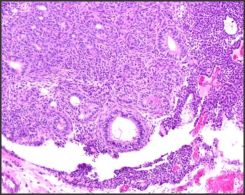 | Photomicrograph of Adenomatold odontogenic Tumor (Lower Magnification)
|
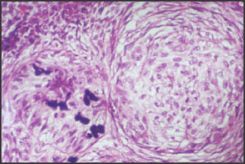 | Photomicrograph of Adenomatold odontogenic Tumor (Higher Magnification)
|
Discussion
Adenomatoid odontogenic tumor (AOT) is a well recognized odontogenic tumor across the world where the histology of tumor does not differ widely [8],[9],[10],[11],[5],[12] It has been estimated from various studies that the AOT accounts for between 2.2 and 7.1 % of all odontogenic tumors in English literature, which gives the tumor a ranking of fourth or fifth among the odontogenic tumors. But in present series, AOT accounts for 15.2 % of odontogenic tumors and ranks second among odontogenic tumors. More than half of the cases (63.3%) in this review occurred in second decade which is in agreement with the literature [1], [2], [3], [15], [18]. The female: male ratio for all AOT cases in this review is 1.9:1. However, Asian AOT cases show a female: male ratio of 2.3:1 compared to non-Asian cases 1.4:1. Hence, our study coincides with study of Asian countries.
The site of occurrence is greater in the maxilla than in the mandible (2.7:1). In contrast to ameloblastoma, this tumor occur more frequently in the anterior portion of the jaws. Concerning the distribution of unerupted permanent teeth in follicular AOT, maxillary canine is involved in most of the cases. Unerupted first and second molars are rarely involved in this review. In contrast to this, China has found equal distribution in maxilla : mandible [2].
The follicular type shows a unilocular radiolucency associated with unerupted tooth, thus mimicking a dentigerous cyst. The extrafollicular type is found between, above or superimposed upon the roots of erupted permanent teeth, leading to the tentative diagnosis of residual, radicular or lateral periodontal cyst. There may be a slight erosion of alveolar bone crest in peripheral AOT as seen in single case in this review. Irrespective of the tumor variants, histology is identical. Although combined AOT/Calcifying Epithelial Odontogenic Tumor cases have been described in the literature [5], [8], [11], [16], [17] but in this review, no such case has been reported.
Since all the variants of AOT show an identical benign biological behaviour, conservative surgical enucleation has proven the treatment modality of choice. In this review, 24 patients were treated with same treatment modality without any recurrence while 6 patients did not report for the treatment.
Conclusion
The distribution and characteristics of Adenomatoid odontogenic tumor (AOT) in this population are similar to the findings found in other populations. This updated review though based on the less number of AOT cases presented, confirms the distinctive, although not pathognomonic clinicopathological profile of the AOT, its worldwide occurrence, and its consistently benign behaviour.
References
1. Philipsen HP, Reichart PA. Adenomatoid odontogenic tumor: facts and figures. Oral Oncol 1999; 35: 125-31.
2. Jing W, Xuan M, Lin Y et al. Odontogenic tumors: a retrospective study of 1642 cases in Chinese population. Int J Oral Maxillofac Surg 2007; 36: 20-5.
3. Lu Y, Xuan M, Takata T et al. Odontogenic tumors. A demographic study of 759 cases in Chinese population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 86: 707-14.
4. Wu PC, Chan KW. A survey of tumors of the jawbones in Hong Kong Chinese. Br J Oral Maxillofac Surg 1985; 23: 92-102.
5. Siar CH, Ng KH. Adenomatoid odontogenic tumor: a survey of 44 new cases in Malaysia. Ann Dent 1986; 45: 11-4.
6. Siar CH, Ng KH. The combined epithelial odontogenic tumor in Malaysians. Br J Oral Maxillofac Surg 1991; 26: 106-9.
7. Okada H, Yamamoto H, Tilakaratne WM. Odontogenic tumors in Sri Lanka: analysis of 226 cases. J Oral Maxillofac Surg 2007; 65: 875-82.
8. Chattopadhya A. Adenomatoid odontogenic tumor. Review of literature and report of 30 cases from India. Indian J Dent Res 1994; 5: 89-95.
9. Leon JE, Mata GM, Fregnani ER et al. Clinico pathological and immunohistochemical study of 39 cases of adenomatoid odontogenic tumor: a multicentric study. Oral Oncol 2005; 41: 835-42.
10. Mendis BRRN, MacDonald DG. Adenomatoid odontogenic tumor. A survey of 21 cases from Sri Lanka. Int J Oral Maxillofacial Surg 1990; 19: 141-3.
11. Philipsen HP, Reichart PA, Zhang KH, Nikai Yu QX. Adenomatoid odontogenic tumor: biologic profile of based on 499 cases. J Oral Pathol Med 1991; 20: 149-58.
12. Swasdison S, Dhanuthai K, Jainkittivong A, Philipsen HP. Adenomatoid odontogenic tumors: an analysis of 67 cases in Thailand. Oral Surg Oral Med Oral Pathol Oral Radio Endod 2008; 105: 210-5.
13. Adeboya ET, Ajike SO, Adekeye EO. A review of 318 odontogenic tumors in Kaduna, Nigeria. J Oral Maxillofac Surg 2005; 63: 811-9.
14. Barnes L, Eveson JW, Reichart P, Sidransky D. (eds) World Health Organization classification of tumors. Pathology and genetics of head and neck tumors. Lyon: IARC Press, 2005; 304-5.
15. Toida M, Hyodo I, Okuda T, Tatematsu N. Adenomatoid odontogenic tumor: report of two cases and survey of 126 cases in Japan. J Oral Maxillofac Surg 1990; 48: 404-8.
16. Philipsen HP, Reichart PA, Siar CH et al. An updated clinical and epidemiological profile of the adenomatoid odontogenic tumor: a collaborative retrospective study. J Oral Pathol Med 2007; 36: 383-93.
17. Kramer IRH, Pindborg JJ, Shear M. Histological typing of odontogenic tumors, 2nd ed. Berlin: Springer Verlag, 1992. |