Introduction
Endodontics has been practiced as early as second or third century BC. The history of endodontics begins in 17th century and since then many advances, developments and research work has been conducted continuously. The technological advances made routinely since the early part of this decade have far exceeded the progress made since the discipline was first recognized as a specialty. The advent of nickel titanium files, rotary instrumentation, “endosonics,” radiovisiography, endoscope, and the clinical microscope are but a few innovations that have changed the way in which endodontics is practiced. This progress has increased both productivity and quality of care. The public's awareness and interest in preserving their teeth are increasing, and cases that heretofore were not attempted are now being successfully managed. On the other hand, the complexity of the cases being treated by both general dentists and endodontists is increasing, with the result that new problems need to be addressed
One of the most common problem that compromise the success of endodontic therapy is Missed canals. These Elusive canals are those that are missed by dentist during endodontic procedure.
A missed canal decreases the prognosis and will most likely result in treatment failure. Locating all of the canals in a multicanal tooth is the best prevention of treatment failure. There are many methods that can be employed to prevent this unfortunate event. This article discusses various methods for detection of these elusive missed canals.
Role Of Radiographs: Buccal-object Rule (Cone Shift)
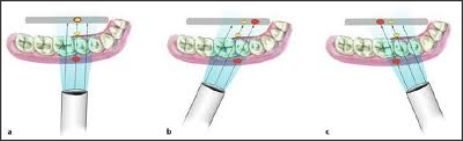
Radiographic examination is an essential component in all aspects of endodontic treatment, from diagnosis and treatment planning to assessing outcome. Radiographs have been conventionally used by dentists for ascertaining the number of canals and for detection of extra canals. Information gained from conventional films and digital periapical radiographs is somewhat limited. In endodontic therapy, it is imperative that the clinician should know the spatial or buccal-lingual relation of an object within the tooth or alveolus. The technique used to identify the spatial relation of an object is called the cone or tube shift technique. Other names for this procedure are the buccal object rule, Clark's rule, and the SLOB (same lingual, opposite buccal) rule. [1] (Fig 1) Proper application of the technique allows the dentist to locate additional canals or roots, to distinguish between objects that have been superimposed and between various types of resorption, to determine the buccal-lingual position of fractures and perforative defects, to locate foreign bodies, and to locate anatomic landmarks in relation to the root apex, such as the mandibular canal.[2], (Fig 2)
 | FIG 2: RADIOGRAPH TAKEN AT A DIFFERENT SHIFT HELPS IN DETECTION OF AN ADDITIONAL ROOT.
 |
 | Fig. 1. Pre-operative photograph showing generalised discolouration of teeth
|
Dental Operating Microscope
The introduction of the dental operating microscope has changed both non-surgical and surgical endodontics. An important aid for location of root canal orifices is the Dental Operating Microscope (DOM).The increased magnification and coaxial illumination decreases the chances of missed canals. In non-surgical endodontics, every challenge existing in the straight portion of the root canal system, even if located in the most apical part, can be easily seen and managed competently under the microscope.[3] (Fig 3,4,5) The DOM enhances clinicians ability to remove dentin with greater precision. Many studies eliciting utility of DOMs for location and negotiation of such elusive missed canals have been conducted.
 | FIG 3: THE ORIGINAL DENTISCOPE
|
 | FIG 4: NEWER DOM
|
 | FIG 5: MAGNIFICATION LOUPES
|
Ultrasonics
Ultrasonics (US) in endodontics has enhanced the quality of treatment and represents an important adjunct in the treatment of difficult cases. Since its introduction, US has become increasingly more useful in applications such as gaining access to canal openings, cleaning and shaping, obturation of root canals, removal of intracanal materials and obstructions, and endodontic surgery.
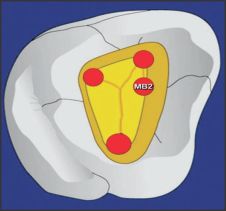
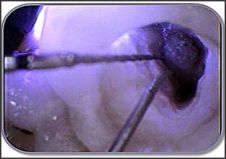
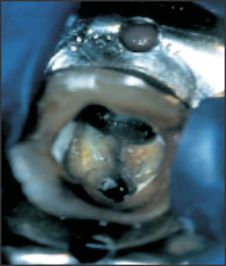
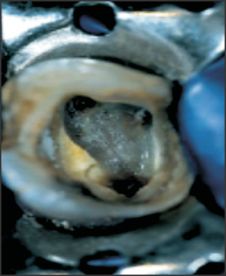
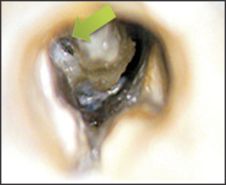
One of the challenges in endodontics is to locate canals in cases in which the orifice has become occluded by secondary dentin or calcified dentin secondary to the placement of restorative materials or pulpotomies. With every access preparation in a calcified tooth, there is the risk of perforating the root or, when incorrectly performed, of complicating each subsequent procedure. Microscopic visualization and ultrasonic instruments are a safe and effective combination to achieve optimal results[6],[7],[8]. In difficult-to-treat teeth such as molars, US has proven to be useful for access preparation, not only for finding canals, but also for reducing the time and the predictability of the treatment [4],[5]. In conventional access procedures, ultrasonic tips are useful for access refinement, location of MB2 canals in upper molars and accessory canals in other teeth, location of calcified canals in any tooth, and removal of attached pulp stones [6],[7],[8]. When locating the MB2 canals in upper molars, US is an excellent means for the removal of secondary dentin on the mesial wall (Fig 6). When searching for hidden canals, one should remember that secondary dentin is generally whitish or opaque, whereas the floor of the pulp chamber is darker and gray in appearance. US works well when breaking through the calcification that covers the canal orifice. A troughing tip is a good choice for this task (Fig 7)
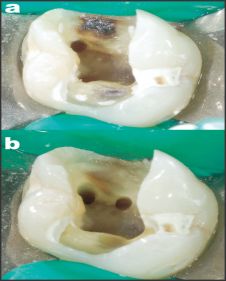 | FIG 6.The orifice of the second mesiobuccal canal (MB2) in an upper firstmolar was located (a) and enlarged (b). Dentine spur at the orifice was effectively eliminated with the use of a diamond-coated ultrasonic tip, thus permitting easy location of the o
|
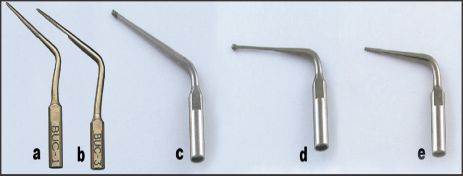 | FIG 7. (a) The BUC-1 is an example of diamond-coated spreader tip of medium length that can be used for gross dentin removal, moving access line angles, cutting a groove in the mesial access wall to drop into MB2 canals, and quickly and carefully unroofin
|
Geometric Techniqus
Traditionally, access cavities have been prepared in relation to the occlusal anatomy. However, complete reliance on the occlusal anatomy is dangerous because this morphology can change as the crown can be destroyed by caries and reconstructed by various restorative materials. Complete dependence on the occlusal anatomy may explain the occurrence of procedural errors like missed canals, perforation etc. Krasner and Rankow utilized geometric techniques to formulate a set of laws to set guidelines for easier location of canal orifices.
Krasner And Rankow Laws[9] (Fig 8)
Law of centrality: The floor of the pulp chamber is always located in the center of the tooth at the level of the CEJ.
Law of concentricity: The walls of the pulp chamber are always concentric to the external surface of the tooth at the level of the CEJ.
Law of the CEJ: The CEJ is the most consistent, repeatable landmark for locating the position of the pulp chamber.
Law of Color Change: The color of the pulp-chamber floor is always darker than the walls.
Law of symmetry 1: Except for maxillary molars, the orifices of the canals are equidistant from a line drawn in a mesial distal direction through the pulp-chamber floor.
Law of symmetry 2: Except for the maxillary molars, the orifices of the canals lie on a line perpendicular to a line drawn in a mesial-distal direction across the center of the floor of the pulp chamber.
Law of orifice location 1: The orifices of the root canals are always located at the junction of the walls and the floor.
Law of orifice location 2: The orifices of the root canals are located at the angles in the floor-wall junction.
Law of orifice location 3: The orifices of the root canals are located at the terminus of the root developmental fusion lines.
 | FIG 8 Law of centrality and Law of concentricity (A) Cut specimen showing the laws of symmetry 1 and 2 and orifice locations 1, 2, and 3. (B) Laws of symmetry 1 and 2 and orifice locations 1, 2, and 3.
|
 | FIG 10: FIBRE OPTIC LIGHT FOR TRANSILLUMINATION
|
Beer And Bauman Technique (Fig 9)
LINE 1: connects MB canal to Palatal canal
LINE 2: Perpendicular to Line 1, at a point one third from intercanal distance of palatal canal, such that the line passes over distobuccal canal
LINE 4: Lies on LINE 3 that deviates 100
Transillumination
Apart from magnification, illumination is an important adjunct for location of canal orifices. Previous sources of illumination could not illuminate site even after reflection. Introduction of transillumination provided by fibreoptics (Fig 10) helped to increase chances of detection of additional canals. (Fig 11 a, b) More over this technique also helps in the assessment of calcifications. (Fig 12)
 | FIG 9: BEER AND BAUMAN TECHNIQUE
|
 | FIG 11(a):Transillumination of pulp floor
|
 | FIG 11(b): Transillumination of MB2 & MB3
|
Dyes
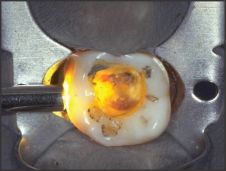
Dyes like methylene blue , Indian ink, Basic Fushchin are also used for location of additional canals. Moreover dyes can also be used for detection of fractures and carious exposure. After use of dye the tooth can be cleaned using 70% isopropyl alcohol. (Fig 13 a, b, c). Dyes provide a road map to detect canals with greater predictability.
 | FIG 12: Transillumination reveals dystrophic calcifications in the pulp chamber.
|
Cone-Beam Computed Tomography
The radiographic interpretation of a potential endodontic pathosis is an integral part of endodontic diagnosis and prognosis assessment. Until 10 years ago, routine dental radiograph consisted of two dimensional imaging. But limitations of conventional radiography promulgated a need for three dimensional imaging, also known as cone-beam computed tomography (CBCT) and cone-beam volumetric tomography (CBVT). The use of these devic es increased in dentistry since 1998. CBCT/ CBVT utilise 3 D view of patients tissues in multitude of planes and assessment of variations in root and root canal anatomy can be accurately detected.
In vivo studies with operating microscopes (Sempira & Hartwell 2000[10]) and conventional radiography (Omer et al. 2004[11]) are undertaken frequently to evaluate tooth anatomy (Fig 14). Previous studies (Tu et al. 2007[12], Scha¨fer et al. 2009[13]) have suggested that three-dimensional radiographic techniques, such as computed tomography (CT) scans, could offer a more accurate method for these investigations. Recently, cone-beam computed tomography (CBCT) images have been found to be useful and accurate in detecting periapical lesions and assessing root canal morphology (Fig 15) (Tsiklakis et al. 2005[14], Nakata et al. 2006[15], Lofthag-Hansen et al. 2007[16], Zhang et al. 2011[17]). CBCT has also been used to estimate the inter-orifice distances of root canals in three-rooted mandibular molars in Taiwanese individuals (Tu et al. 2009[18]). As an emerging technology in endodontics, CBCT, with its lower radiation and higher resolution than traditional CT scans (Arai et al. 2000[19], Patel 2009[20], Patel et al. 2009[21]), has produced valid root and canal details in three dimensions for diagnosis and prognosis in the context of endodontic therapy (Cotton et al. 2007[22], Matherne et al. 2008[23]).
 | FIG 13 a: Use of dye Before Staining
|
 | FIG 13 b: After Staining
|
Clinical Significance
It is difficult to detect the third roots of mandibular molars with conventional radiography because the images of the roots overlap and the roots themselves are narrow. Moreover, branching of the canals may not be obvious, especially if they are fine. An angled view (vertically and horizontally) may be helpful (Cooke & Cox 1979[24]), but achieving such a view is often difficult. If adjacent teeth, restorations or implants are present, there is even more overlap, reducing the clarity of the radiographic image. When root canal treatment is considered, special attention to the extra distolingual roots is necessary, especially when they are smaller than the other roots and are curved (Vertucci et al. 2006[25]). Clearly, the failure to locate and negotiate the narrow additional distolingual canal may result in treatment failure (Gulabivala et al. 2002[26]).
Other Aids
Munce discovery burs (Fig 16), Endodontic explorers, Rod lens endoscope and orascope (Fig 17) , Sodium hypochlorite champagne bubble test (Fig 18), loupes etc are commonly used for detection of missed canals.
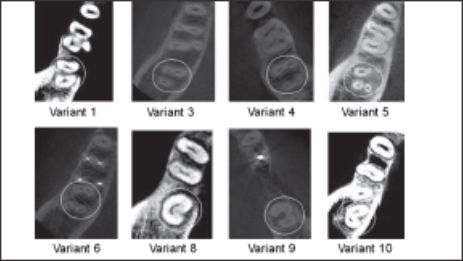 | FIG 14 Cone-beam computed tomography images showing the categorisation of the eight variants in mandibular second molars found . The white circles indicate the examined tooth. (Courtsey: Zhang et al.2011 Chinese root canal morphology)
|
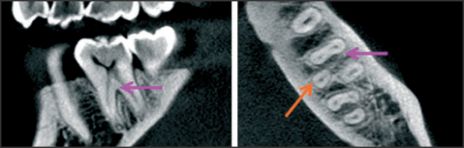 | FIG 15:Cross-sectional cone-beam computed tomography image of a mandibular first molar with a clearly distinguishable distolingual root. The purple arrows denote the mandibular first molar and the orange arrows denote the distolingual root. (Courtsey: Zha
|
 | FIG 13 c: MB2 Identified
|
 | FIG 16: MUNCE DISCOVERY BURS
|
 | FIG 17: ROD LENS ENDOSCOPE AND ORASCOPE
|
 | FIG 18: SODIUM HYPOCHLORITE CHAMPAGNE BUBBLE TEST
|
Conclusion
The concept that each tooth has a fixed number of root and root canals is now obsolete and it is the responsibility of dentist to look for those Elusive canals that might get missed leading to poor prognosis of treatment. In past decade or so dentistry especially the specialty of endodontics has witnessed a sea of change with the introduction of newer and improved armamentarium that has made the treatment more predictable.
References
1. American Dental Association: Your teeth can be saved by endodontic (root canal) treatment, Chicago, 1985, The Association.
2. Glickman GN, and Schwartz SF: Preparation for treatment. In CohenS, and Burns RC. eds: Pathways of the pulp, ed 5, St. Louis, 1991, Times Mirror/Mosby College Publishing.
3. Gary B. Carr, Arnaldo Castellucci. The Use of the Operating Microscope in Endodontics. Endod 2004; 31(2):32-33.
4. Clark D. The operating microscope and ultrasonics: a perfect marriage. Dent Today 2004;23:74-81.
5. Buchanan LS. Innovations in endodontics instruments and techniques: how they simplify treatment. Dent Today 2002;21:52- 61.
6. Sempira HN, Hartwell GR. Frequency of second mesiobuccal canals in maxillary molars as determined by use of an operating microscope: a clinical study. J Endod 2000;26:673- 4.
7. Gorduysus MO, Gorduysus M, Friedman S. Operating microscope improves negotiation of second mesiobuccal canals in maxillary molars. J Endod 2001;27:683- 6.
8. Rampado ME, Tjaderhane L, Friedman S, Hamstra SJ. The benefit of the operating microscope for access cavity preparation by undergraduate students. J Endod 2004;30:863-7.
9. Krasner and Rankow Anatomy of the Pulp-Chamber Floor. . J Endod 2004, 30(1); 5-17.
10. Sempira HN, Hartwell GR .Frequency of second mesiobuccal canals in maxillary molars as determined by use of an operating microscope: a clinical study. J Endod 2000; 26:673-4.
11. Omer OE, Al Shalabi RM, Jennings M, Glennon J, Claffey NM A comparison between clearing and radiographic techniques in the study of the root-canal anatomy of maxillary first and second molars. Int Endod J 2004; 37: 291-6.
12. Tu MG, Tsai CC, Jou MJ et al. Prevalence of threerooted mandibular first molars among Taiwanese individuals. J Endod 2007; 33: 1163-6.
13. Scha¨fer E, Breuer D, Janzen S The prevalence of threerooted mandibular permanent first molars in a German population. J Endod 2009; 35:202-5.
14. Tsiklakis K, Donta C, Gavala S, Karayianni K, Kamenopoulou V, Hourdakis CJ .Dose reduction in maxillofacial imaging using low dose Cone Beam CT. European Journal of Radiology 2005; 56:413-7.
15. Nakata K, Naitoh M, Izumi M, Inamoto K, Ariji E, Nakamura H. Effectiveness of dental computed tomography in diagnostic imaging of periradicular lesion of each root of a multirooted tooth: a case report. J Endod 2006 ;32:583-7.
16. Lofthag-Hansen S, Huumonen S, Gro¨ndahl K, Gro¨ndahl HG Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surgery Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology 2007;103:114-9.
17. Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PMH .Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J 2011; 44:162-9.
18. Tu MG, Huang HL, Hsue SS et al. Detection of permanent three-rooted mandibular first molars by cone beam computed tomography imaging in Taiwanese individuals. J Endod 2009; 35: 503-7.
19. Arai Y, Tammisalo E, Iwai K, Hashimoto K, Shinoda K .Fundamental efficiency of limited cone-beam X-ray CT (3DX multi image micro CT) for practical use. Dental Radiology 2000; 40: 145-54.
20. Patel S .New dimensions in endodontic imaging: part 2. Cone beam computed tomography. Int Endod J 2009;42:463-75.
21. Patel S, Dawood A, Wilson R, Horner K, Mannocci F .The detection and management of root resorption lesions using intraoral radiography and cone beam computed tomography: an in vivo investigation. Int Endod J 2009; 42: 831-8.
22. Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applications of cone-beam volumetric tomography. J Endod 2007; 33: 1121-32
23. Matherne RP, Angelopoulos C, Kulild JC, Tira D. Use of cone-beam computed tomography to identify root canal systems in vitro. J Endod 2008; 34: 87-9
24. Cox FL .C-shaped canal configurations in mandibular molars. J Am Dent Asso 1979; 99: 836-9.
25. Vertucci FJ, Haddix JE, Britto LR .Tooth morphology and access cavity preparation. In: Cohen S, Hargreaves KM, eds. Pathways of the Pulp, 9th edn. St Louis: CV Mosby, pp. 149-232.
26. Gulabivala K, Opasanon A, Ng YL, Alavi A .Root and canal morphology of Thai mandibular molars. Int Endod J 2002; 35: 56-62. |