Introduction
Occurrence of Impaction of teeth in maxilla is third molar, canine, first and second premolars. [1],[2]. Impaction of maxillary central incisor is not one of the commonest occurrences [3]. Though rare, treatment for them is one of the most challenging. As max central incisor is the most visible tooth in the oral cavity, management of this demands high aesthetic standards with utmost care to retain the vitality of the tooth.
Size and shape of central incisor does not allow it to be extracted and camouflaged with lateral incisor. The cervical incisal length, faciolingual curvature distal curvature on the cervical third of facial surface does not allow it to mimic central incisor [4].
If the impacted central incisor is extracted and replaced by an implant, the drawbacks being; a good healthy tooth is lost, treatment has to be delayed as after 18 years of age, if done earlier shortening of implant tooth is common.
So the best treatment possible is to orthodontically move the impacted tooth into good occlusion and alignment so a very conservative approach but with best result [5]. Though vitality of tooth has to be watched carefully, and dilacerations may appear [6],[7].
Impacted tooth sometimes may erupt spontaneously if the causative factor such as supernumery tooth, retained deciduous is removed or space is made available for the eruption of the impeding tooth. But the time taken for the eruption is very long and the tooth neither may or may nor erupt on its own depending on its site and angulations of impaction [8]. There are very few records available of successfully treated impacted central incisors.
Surgical repositioning has been the treatment of choice. This may lead to devitalisation of the tooth involved or resorbtion of tooth after a period of time.
Case Study
A healthy 9 year old male patient referred by a general dentist in a private hospital reported to the clinic. The boy had a non erupted maxillary left central incisor, with no other relevant medical history / trauma. Parents were concerned with non eruption of the tooth and compromised aesthetics.
Clinical Examination
Oral examination revealed non erupted left maxillary central incisor, on palpation incisal edge of the incisor could be palpated high up in the labial vestibule. Maxillary right central incisor and maxillary lateral incisors were already erupted; slightly obliterating the space for central incisor. There was deficiency of space for the eruption of impacted central incisor due to drifting of adjacent teeth into the non erupted tooth space. No other abnormal feature was found.
Radiographic Examination
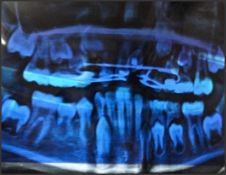
Panoramic radiograph (Fig. 1) revealed an un erupted maxillary left central incisor, lying horizontally high up in the alveolar ridge with facial surface towards nasal floor, right maxillary central and left lateral incisor erupted with 2/3rd root formed. Right lateral incisor in the process of eruption with half of the root formed. Right central incisor and left lateral incisor tilted into the space for left central incisor partially occupying the right central incisor space, left and right maxillary deciduous canine were present.
 | Fig. 1. Showing horizontally impacted maxillary left central incisor
 |
Treatment
Deciduous canines were extracted, flap over the maxillary left central incisor was raised and bracket bonded to the impacted maxillary incisor, flap resutured and wire attached to the bracket left coming out of the flap. Fixed treatment started in upper arch with niti palatal expander given its arms extending up to left lateral incisor. The wire from max left incisor was tied to the bridge of niti palatal expander (Fig 2). Patient was asked to put mild pressure on his upper lip above the 21 crown 4-5 times daily.
 | Fig 2. Palatal expander in place with ligature wire from left central incisor tied to its bridge.
|
The treatment plan consisted of using closed eruption, as this is cited to be the best choice in such cases than excisional gingevectomy and apically positioned flap technique on account of better aesthetic results [9].
Full thickness flap was raised, there was no bony tissue overlying the crown. A Begg's bracket was bonded on to the facial surface of the tooth and a stainless steel ligature wire was tied to the vertical slot and left extended outside the flap. Flap was resutured and closed eruption technique followed so as not to irritate the labial mucosa, Begg's bracket was chosen for its small size and vertical slot allowed ligature wire to be tied without it being dislodged during the treatment duration.
The extending wire was lightly tied to the bridge of niti palatal expander. The lateral arms of the expander rested on the lateral and right central incisor and contacted their proximal surface to assist the opening up of the 21 space[5]. The deciduous canines were also extracted to create space for the 21. Begg's bracket was also bonded on the 11 and 22 so as to engage a wire on them on a later stage. As of now we did not want to disturb the eruption of canines.
Patient was asked to regularly put mild pressure on the labial surface (palpable) of 21, as to help guide the incisor towards occlusion.
The ligature wire tied to the 21 was regularly tightened slightly. 21 oriented itself in a vertical direction within six months, though still did not emerge into the oral cavity. By now the Begg's bracket could be felt in a vertical direction above the alveolar ridge. This can be seen on radiographic examination (Fig 3). No dilacerations or resorbtion can be seen.
 | Fig 3. Central incisor in vertical position
|
The tooth started erupting within 10th month of treatment (Fig 4).
 | Fig. 4. Impacted maxillary incisor emerging in the oral cavity
|
Whole of the crown was now visible in the oral cavity with good aesthetic results. (Fig. 5).
 | Fig. 5. Fully erupted left central incisor
|
Further treatment was discontinued after six months of retention as canines were still to erupt. Patient had class I molar relationship. Parents did not want further treatment and were satisfied with the result. 21 was vital and did not show any dilacerations (Fig. 6).
 | Fig 6. impacted incisor brought into alignment, canine about to erupt
|
Discussion
There are not many reported cases in the literature of treatment of horizontally impacted maxillary central incisor by orthodontic repositioning.
In the present case as the patient was diagnosed quite early in mixed dentition stage, the treatment of choice was to retain the incisor and bring it into a right occlusion and alignment with the orthodontic treatment.[6]
The choice of treatment was with closed eruption. This helped to reduce infection, irritation of labial mucosa by bracket placed [9].
Begg's bracket was chosen because of its small size [10] and vertical slot which helped to secure the ligature wire.
The bracket was bonded to the facial surface because of better bonding in this area as compared to lingual anatomy; also the wire from the facial position did not impinge directly on the palatal mucosa.
The use of ligature wire was for controlled amount of force which we did not want to exceed. And also elastics and e-chain were impinging on palatal mucosa and would collect more of plaque.
Slight amount of regular pressure by the patient as regular exercise achieved the desired result of up righting the central incisor.
The niti palatal expander with activated arms gained the desired space for eruption of 21.
Similarly the deciduous canine extraction gave us enough space for eruption of 21.
Further treatment after eruption and alignment of 21 was discontinued as canines were still to erupt and patient did not have any other malocclusion. Parents were satisfied with the result and did not want full fixed treatment at this stage.
Low magnitude of force was applied to the tooth. The force was merely used to align the tooth in natural position and the erupting pressure of the tooth brought the tooth into occlusion.
Conclusion
In the present case it can be well concluded that the age of patient plays a vital role in the treatment of impacted maxillary incisor.
Horizontally Impacted maxillary incisor if diagnosed in early mixed dentition period with no dilacerations of root present, treatment of choice should be to orthodontically reposition the tooth, and with closed eruption technique followed
The amount of force applied should be minimal in nature and eruptive forces of the developing root of the tooth should be used to the maximum
References
1. Alling CC, Helfrick JF, Alling RD, Impacted Teeth, 1st ed philadelphia: Saunders, 1993:2.
2. Grover PS, Lorton L. The incidence of Unerupted permanent teeth and related clini Cases. Oral surg oral med oral path 1985;59:420-425.
3. Kamat, S. S. , G. S. Kumar , V. Raghunath , and K. P. Rekha . Permanent maxillary central incisor impaction: report of two cases. Quintessence Int 2003. 34:50-52
4. Ash M, Nelson SJ. Wheelers dental anatomy physiology, and occlusion, eight edition 149-169.
5. Eiji Tanaka, Takuro Hasegawa, Koichi Hanaoka, Kiyoshi Yoneno, Eka Matsumoto, Diego Dalla-Bona, Eizo Yamano, Yohei Suekawa, Mineo Watanabe, and Kazuo Tanne (2006) Severe Crowding and a Dilacerated Maxillary Central Incisor in an Adolescent. The Angle Orthodontist: May 2006, Vol. 76, No. 3, pp. 510-518.
6. Setsuko Uematsu, Takashi Uematsu, Kiyofumi Furusawa, Toshio Deguchi, and Saburo Kurihara (2004) Orthodontic Treatment of an Impacted Dilacerated Maxillary Central Incisor Combined with Surgical Exposure and Apicoectomy. The Angle Orthodontist: February 2004, Vol. 74, No. 1, pp. 132-136.
7. Dalia Smailiene, Antanas Sidlauskas, Jevgenija Bucinskiene Stomatolog ija, Baltic Dental and Maxil lofacial Journal, 2006, Vol. 8., No. 4. 10 3 Impaction of the central maxillary incisor associated withsupernumerary teeth: Initial position and spontaneous eruption timing.
8. Becker, A. , I. Brin , Y. Ben-Bassat , Y. Zilberman , and S. Chaushu . Closed-eruption surgical technique for impacted maxillary incisors: a postorthodontic periodontal evaluation. Am J Orthod Dentofacial Orthop 2002. 122:9-14.
9. Chawla HS, Kapur A. Orthodontic management of faciolingual horizontally impacted maxillary central incisor. J Indian Soc Pedod Prev Dent 2009;27:65-9.
10. Becker A. Early treatment for impacted maxillary incisors.Am J Orthod Dentofac Orthop 2002; 121( 6): 586. |