Introduction
Swelling in the gingival or alveolar mucosal region is frequently encountered in dental practice. It is most commonly associated with periodontal or root canal infection, apart from them some other root structure abnormalities, such as palatoradicular groove, root fracture and cemental tears can be associated with it.[2] Vertical root fractures (VRF) are diagnostic challenge to clinicians because of their varied presentation.[15] VRF is typically associated with previous non-surgical root canal treatment and accompanied by periodontal defect.[13] Cemental or cementodentinal tear are specific type of root fracture which are described as 'Complete separation along the cementodental border or a partial split within the cemental tissues along an incremental line'.[11] From the limited number of case reported earlier central incisors and premolars seems to be the major affected teeth.[5] The most frequent suggested causes are occlusal trauma and aging.[9], [6] The prevalence of cemental tears is still not known; this is possibly owing to difficult diagnoses of cemental tears leading to limited case reported in the literature.[1]
The purpose of this article is to bring forward a case of cemental tear misdiagnosis and further consequences of it in relation to a maxillary left first premolar.
Case report
A 32 year old male patient has experienced pain in the left upper back region jaw for past 5 days. Three days back he visited to a local dentist for the same. Periapical radiography was performed (Fig 1), and a foreign body was removed from the interdental area of first and second premolar. The removed fragment was handed over to the patient and medication was prescribed. The next morning that is 4 days back the patient reported to the same dentist with pain and intra oral swelling leading to the obliteration of buccal vestibule in relation to the two premolars. The patient was then referred to the Department of conservative Dentistry and Endodontics, Himachal Institute of Dental Sciences, Paonta Sahib for further treatment. The patient visited the department along with the removed fragment which he had taken from the dentist wrapped in cotton. On clinical examination the vestibule presented with a fluctuant, palpebral, soft and edematous buccal swelling in relation to the two premolars. On clinical probing no sign of caries was observed on the first premolar and probing around the tooth was within the normal limits (<3 mm), vitality tests were performed on the first premolar and positive results were obtained for the first premolar. There was also presence of two porcelain-fused- to-metal crowns in the second premolar and maxillary 1st molar. Periapical radiography was carried out to assess the two crowned teeth (Fig 2). Root canal obturation with an acceptable quality was found from the periapical radiograph. Careful examination of the periapical radiograph detected a radiolucent concavity in the distal aspect of 1st premolar. Based on the findings from the current radiograph and the radiograph before segment removal, a tentative diagnosis of a cemental tear was made. A non- surgical endodontic treatment approach was planned for the patient and root can treatment was carried out. No discharge was seen through the canals during the cleaning and shaping procedure so a decision of single visit endodontics was made and the canal were obturated using AH Plus Sealer and gutta percha cones. The patient was sent back and recalled after two days for further evaluation. At the same time the fragment which patient has brought was sent for histo-pathological examination.
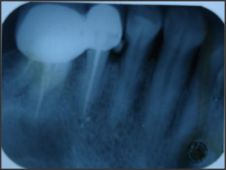 | Fig. 1- Radiograph with detach fragment (pre-operative)
 |
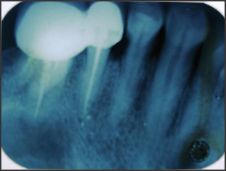 | Fig. 2- Radiograph after fragment was removed
|
After two days the patient reported asymptomatic to us. On clinical examination the buccal vestibular swelling was not present and tooth was not tender.by now the histo-pathological report has confirmed the fragment to be a cemental tear so exploratory surgery and closure of defect was planned. Under local anesthesia, an envelope flap was lifted and distal aspect of the first premolar was exposed. Curettage was performed and after the removal of granulation tissue the defect was closed with MTA which was then covered with GIC on top of MTA. Radiographic cross checking was performed (Fig.3), Flap was closed sutures were placed. After one week patient follow up was done, patient was asymptomatic and healing was satisfactory so the sutures were removed.
 | Fig. 3- post operative radiograph
|
Discussion
The present case of cemental tear is unusual in nature owing to the fact that it is occurring in young male and at the level of cervical third of the root, which is contradictory to the fact that they occur commonly in the patients older than 60 years (72%) and in the middle third of root (45.3%), and 41.5% over the apical region.[8] The probing depth being within the normal limits can be attributed to the fact that the fragment was removed two days back and healing of the area was satisfactory. Other findings before the surgery like positive vitality testing,[7] and during the surgery like presence of granulation tissue at the fracture site are in accordance with the published data.[8]
Age related changes, heavy occlusal forces and increased thickness, mineralization and brittleness of cementum are suggested to be the major etiologic factors of cemental tears.[12]. The average age of patients with cemental tear is between 50 to 79 years,[3] but cemental tear can occur in young adult also.[14] As the patient was young individual, thus the reduction in fatigue strength of dentine was ruled as a possible cause for the tear. In the present case sudden occlusal trauma or occlusal overloading can be considered as a potential etiologic cause for the cemental tear which is one of the etiologic factors for cemental tear.[10]
Diagnosis of cemental and cementodentinal tear is difficult based on history taking and clinical examination. Radiographic examination can be helpful in some cases when displacement of the detach root fragment is evident as seen in this case. Therefore when a suspected fracture line is detected in radiograph, and when the swelling or sinus tract is present along with it, additional radiographs have to be taken to check for real root fracture or cemental tears.
The long term prognosis of teeth with cemental or cementodentinal tear is not predictable.[17] Previous studies have shown that teeth treated for cemental tear with many different approaches are finally extracted.[14] However with the availability of newer and better materials like MTA the treatment prognosis can be improved. In the present case the defect was curettage and clean and restored with MTA[16] and followed by application of GIC.[4]
Cemental tears may present a diagnostic challenge, although rare cemental tear may be considered in differential diagnosis when there is persistent pain on lateral percussion accompanied by presence of swelling with no known cause from the occlusal surface.
References
1. Camargo P M, Pirih F Q M, Wolinsky L E, Lekovic N, Kamrath H, White S N. Clinical repair of an osseous defect associated with a cemental tear: a case report. Int J Periodont Restor Dent 2003; 23: 79-85.
2. Chan C P, Lin C P, Tseng S C, Jeng J H. Vertical root fracture in endodontically versus nonendodontically treated teeth: a survey of 315 cases in chinese patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999; 87: 504-7
3. Chou J, Rawal Y B, O'Neill J R, Tatakis D N. Cementodentinal tear: a case report with 7 year follow up J Periododntol 2004; 71: 1761-6
4. Eid AA, Komabayashi T, Watanabe E, Shiraishi T, Watanabe I. Characterzation of the mineral trioxide aggregate-resin modified glass ionomer cement interface in different setting conditions. J Endod 2012; 38(8): 1126-9
5. Haney J M, Leknes K N, Lie T, Selvig K A, Wikesjo U M E. Cemental tear related to rapid periodontal breakdown: a case report. J Periodontol 1992; 63: 20-4
6. Haney J M, Leknes KN, Lie T, Selvig KA, Wiksejo UM. Cemental tear related to rapid periodontal breakdown: a case report J Periodontal 1992; 63: 220-4
7. Hsueh-Jen Lin, Chiu-Po Chan, Chu-Yen Yang, Chen-Tsai Wu, Yi-Ling Tsai, Chi-Chia Huang, Kuen-Dah Yang, Chiu-Chun Lin, Shu-Hui Chang, Jiiang-Huei Jeng. Cemental tear: clinical characteristics and its predisposing factors J Endod2011;37(5): 611-8
8. Hsueh-Jen Lin, Shu-Hui Chang, Mei-Chi Chang, Yi-Ling Tsai, Chun-Pin Chiang, Chiu-Po Chan, Jiiang-Huei Jeng. Clinical fracture sites, morphologicand histopathologic characteristics of cemental tear: Role in endodontic lesions J Endod 2012; 38(8): 1058-62
9. Ishikawa I, Oda S, Hayashi J, Arakawa S. Cervical vemental tears in older patients with adult periodontitis. case reports J Periodontol 1996;67: 15-20
10. Leknes K N. the influence anatomic and iatrogenic root surface characterstics on bacterial colonization and periodontal destruction: a review. J Periodontol 1997; 68:507-16
11. Likens Kn, Lie T, Selvig K A. Cemental tear: a risk factor in periodontal attachment los. J Periodontol 1996; 67: 583-8
12. Marquam B. Atypical localized deep pocket due to a cemental tear: a case report. J Contemp Dent Pract 2003; 4: 52-64
13. Michael J Tulkki, Michael K Baisden, Scott B McClanahan. Cemental tear: A case report of a rare root fracture J Endod 2006; 32: 1005-7
14. Stewart M L, McClanahan SB. Cemental tear: a case report Internat Endod J 2006; 39: 81-6
15. Tames A, Fuess Z, Lustig J, Kaplavi J. An evaluation of endodontically treated vertically fracture teeth. J Endod 1999; 25: 506-8
16. Tien-Chun Kuo, Ya-An Cheng, Chun-Pin Lin. Clinical management of severe root resorption Chin Dent J 2005; 24(1): 59-64
17. Tseng-fang Tai, Chun-Pin Chiang, Chun-Pin Lin, Chiu-Chun Lin, Jiiang-Huei Jeng. Persistent endodontic lesion due to complex cementodentinal tears in maxillary central incisor-a case report Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 103: e55-e60 |