Introduction:
Ankyloglossia originates from the Greek words ''agkilos" (curved) and ''glossa" (tongue).[1] Ankyloglossia, commonly known as tongue tie, is a congenital oral anomaly which may decrease the mobility of the tongue tip and is caused by an unusually short, thick lingual frenulum which is a membrane connecting the underside of the tongue to the floor of the mouth. The first use of the term ankyloglossia in the medical literature dates back to the 1960s, when Wallacedefined tongue-tie as "a condition in which the tip of the tongue cannot be protruded beyond the lower incisor teeth because of a short frenulum linguae, often containing scar tissue." [2]
Ankyloglossia varies in degree of severity from mild cases, characterized by mucous membrane bands to complete ankyloglossia whereby the tongue is tethered to the floor of the mouth. Ankyloglossia, or tongue-tie, can be observed in neonates, children, or adults.[3]
Classification
Several classifications have been proposed, but none have been universally accepted. (Table Classification)
Case Report:
A six year old boy's parents reported to our clinic after noticing some abnormalities during speech and mastication of food. The chief complaint of the pt was difficulty in speaking and mastication.
Clinical examination revealed a thick fibrous lingual frenulum attachment causing restriction in tongue movement. [Fig.1] Provocation test showed restriction of protrusive and lateral movements of tongue. Patient showed inability to touch tip of the tongue over the palatal region.
 | Figure 1 : Preoperative intraoral view
 |
Heamatological investigations were performed which showed no positive findings. Treatment plan was discussed with patient's parents and after taking consent of the parents frenectomy was planned. Under infiltration anesthesia, a horizontal incision through the frenum was made, the tongue being held upwards so that the frenum is stretched. The wound margins are gently undermined with curved scissors and the wound is transformed into a vertical one by suturing it from left to right. [Fig.2]
 | Figure 2 : Showing Placement of sutures
|
Discussion:
Ankyloglossia is a congenital anomaly characterized by an abnormally short lingual frenulum. The condition is the result of a failure in cellular degeneration leading to a much longer anchor between the floor of the mouth and the tongue.[8] Newborns with tongue tie are often diagnosed and treated by paediatricians .[9],[10]
Congenital oral adhesions may pose both esthetic and functional disturbing ailments to children. Most of them are benign, easily cured and may be treated as soon as possible in the dental office.[11]
The pathogenesis of ankyloglossia is not known. Ankyloglossia can be a part of certain rare syndromes such as X-linked cleft palate and van der Woude syndrome. Most often ankyloglossia is seen as an isolated finding in an otherwise normal child. Maternal cocaine use is reported to increase the risk of ankyloglossia three times. [12]
A significant association between frenal involvement and gingival recession has been reported in the literature.[13]
For many years, the subject of ankyloglossia has been controversial with practitioners of many specialties having widely different views regarding its significance and management. In many individuals, ankyloglossia is asymptomatic; the condition may resolve spontaneously or affected individuals may learn to compensate adequately for their decreased lingual mobility. Some individuals, however, benefit from surgical intervention for their tongue-tie. [14],[15]
Surgical techniques for the therapy of tongue-ties can be through three procedures. 1) Frenotomy is a simple cutting of the frenulum (of neonates). 2) Frenectomy is defined as complete excision, i.e., removal of the whole frenulum (at or after 6 months of age). 3) Frenuloplasty involves various methods to release the tongue-tie and correct the anatomic situation. Along with surgical intervention, revision of the frenum by LASER[16] and revision by electrocautery[17] using a local anesthetic have also been described in literature.
The case presented in this paper was treated with frenectomy and postoperatively significant improvement was noticed during speech and mastication. [Fig.3]
 | Figure 3 : Postoperative View
|
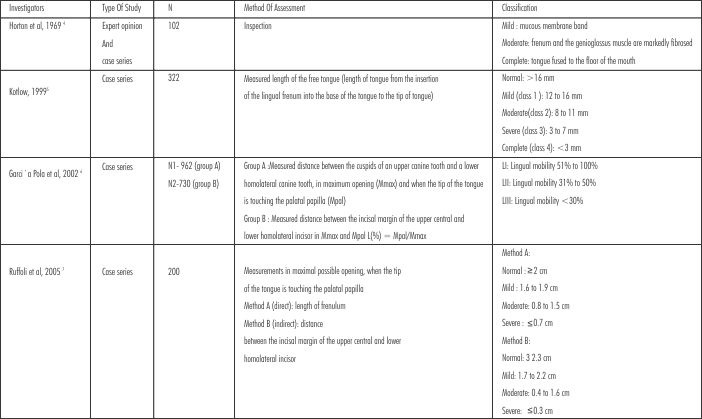 | Classification Table
|
Conclusion
After surgery, the tongue could make wide range of movements including tip-elevation, grooving, and protrusion. Speech and masticatiory functions of the patient were also improved after frenectomy.
References:
1) Suter VGA and Bornstein MM. Ankyloglossia: Facts and Myths in Diagnosis and Treatment. J Periodontol 2009;80:1204-1219.
2) Tanay V. Chaubal and Mala Baburaj Dixit. Ankyloglossia and its management J Indian Soc Periodontol. 2011 Jul-Sep; 15(3): 270-272.Ankyloglossia and its management
3) Harsha M. Babu. Surgical Management of Ankyloglossia - A Case Report. International Journal of Contemporary Dentistry 2010 Nov; 1(2):58-61.
4) Horton CE, Crawford HH, Adamson JE, Ashbell TS. Tongue-tie. Cleft Palate J 1969;6:8-23
5) Kotlow LA. Ankyloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence Int 1999;30: 259-262.
6) Garcia Pola MJ, Gonzalez Garcia M, Garcia Martin JM, Gallas M, Seoane Leston J. A study of pathology associated with short lingual frenum. ASDC J Dent Child 2002; 69:59-62.
7) Ruffoli R, Giambelluca MA, Scavuzzo MC, et al. Ankyloglossia: A morphofunctional investigation in children. Oral Dis 2005; 11:170-174.
8) Klockars T, Pitkaranta A. familial ankyloglossia. Int J Pediatr otorhinolaryngol 2007;71:1321-43
9) Nicholson WL. Tongue-tie (ankyloglossia) associated with breastfeeding problems. J Hum Lact 1991;7:82-4.
10) Morowati S, Yasini M, Ranjbar R, Peivandi A A, and Ghadami M. Familial Ankyloglossia (Tongue-tie): A Case Report. Acta Medica Iranica 2010; 48:123-124.
11) Naimer SA, Biton A, Vardy D, Zvulunov A. Office treatment of congenital ankyloglossia. Med Sci Monit 2003;9:CR432-5.
12) Harris EF, Friend GW, Tolley EA. Enhanced prevalence of ankyloglossia with maternal cocaine use. Cleft Palate Craniofac J 1992;29:72-76.
13) Trott JR, Love B. An analysis of localized gingival recession in 766 Winnipeg High School students. Dent Pract Dent Rec 1966;16:209-213.
14) Kotlow LA. Ankyloglossia (tongue-tie): A diagnostic and treatment quandary. Quintessence Intl.1999;30:259-62.
15) Ayer FJ, Hilton LM. Treatment of ankyloglossia: Report of a case. ASDC J Dent Child. 1977;44:69-71.
16) Kotlow L A. Using the ERBIUM:YAG LASER to correct an abnormal frenum attachment in newborns. The Journal of the academy of LASER Dentistry. 2004;12:22-23.
17) Tuli A, Singh A. Monopolar diathermy used for correction of ankyloglossia. J Indian Soc Pedod Prev Dent 2010;28:130-133. |