Introduction
Dental anomalies have been known to occur in man due to variety of genetic and environmental factors. Supernumerary teeth or hyperdontia is comparatively infrequent developmental alteration [1].Brook found the incidence of supernumerary teeth in primary dentition is 0.8% and in permanent dentition it is 2.1%. The prevalence of supernumerary teeth in Caucasians is between 1% to 3%, out of which 76% to 86% of cases represent only single tooth hyperdontia, with 2 supernumerary teeth noted in 2%-20% and three or more extra teeth in only 1% of the cases [2]. Most cases are found in association with syndromes including apert, Cleidocranial dysplasia, Crouzon, curtius, Gardners, Nance -Horan, Laband, Klippel-Trenaunay- weber, Fucosidosis and cleft lip and palate. The frequency of supernumerary teeth with unilateral cleft lip and palate is 22.2% [3].Gardner's syndrome is associated with a single gene pleiotropism autosomal dominant in nature. 45% of the patients with multiple supernumerary teeth have premalignant intestinal polyposis and 27% out of which may present with intestinal carcinoma associated with this syndrome[2].It has been reported that the prevalence for non syndrome associated multiple supernumerary teeth is less than 1%, So there is always a high suspicion for syndrome association in patients with multiple supernumeraries. The male to female ratio has been reported as 9:2 by Yusof. [2]
The exact aetiology of supernumerary teeth is still obscure although many theories have been proposed. Two popularly accepted theories are: the dichotomy theory of tooth germs states that the tooth bud splits into two equal or different sized parts, resulting in two teeth of equal size or one normal and one dimorphic tooth respectively. Localized and independent hyperactivity of dental lamina is the other accepted theory, which suggests supernumerary teeth are formed as a result of local, inde-pendent, conditioned hyperactivity of dental lamina. Supernumerary teeth can be classified into Mesiodens - present in the incisor region, Paramolars - present beside a molar, Disto-molars - present distal to the last molar, Parapremolars - present beside a premolar which can be Conical, Tuberculate, supplemental or Odontome [4],[5]. Supernumeraries may cause failure of eruption of tooth-The presence of a supernumerary tooth is the most common cause for the failure of eruption of a maxillary central incisor. Displacement The presence of a supernumerary tooth may cause displacement of a permanent tooth. The degree of displacement may vary from a mild rotation to complete displacement. Crowding Erupted supplemental teeth most often causes crowding. A supplemental lateral incisor may cause crowding in the upper anterior region. Pathology Dentigerous cyst formation is another problem that may be associated with supernumerary teeth. Primosch reported an enlarged follicular sac in 30% of cases, but histological evidence of cyst formation was found in only 4 to 9% of cases [5].
Case Report
A 25 years old male came in the Depatment of Periodontology at HP Govt. dental college, Shimla (HP) with chief complaint of Bleeding gums and diffuse pain in the upper jaw and spontaneous eruption of teeth below the tongue. On extraoral examination no significant facial asymmetry was noticed. Intraoral examination revealed that the patient had 5 extra teeth, 1 small erupted conical tooth in the palatal aspect of 15 and 16 , 2 small tuberculate in the lingual aspect of 34 and 35 and 2 similar small tuberculate in the lingual aspect of 44 and 45. No supernumerary teeth were present in the second quadarant of the mouth. All 5 extra teeth were partially erupted in the oral cavity with rudimentary roots whereas crowns were well calcified. None of the permanent tooth was found to be missing as the patient did not show any abnormal systemic manifestations, all the syndromes were ruled out.Fig-1, 2
 | Figure 1
 |
 | Figure 2
|
Investigations
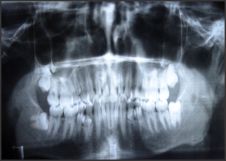
Orthopantomogram was taken to rule out any other supernumerary teeth present in the arches And to rule out tooth fusion or germination of the supernumerary tooth with the permanent tooth .Diagnostic casts were made in order to plan the surgical procedure and to evaluate the need of bone removal and bone graft placement at the time of surgery.Fig-3
 | Figure 3
|
Periodontal Treatment
Comprehensive periodontal treatment was instituted. Complete oral prophylaxis including supragingival and subgingival scaling and subgingival curettage was performed. Frequent subgingival irrigations were done with chlorhexidine gluconate(0.12%) , deep periodontal pockets were impregnated with metronidazol gel (25%) and patient was kept on antihypersensitivity mouth wash (potassium nitrate 4%) to be used twice daily half an hour after brushing and antihypersensitivity tooth paste(stannous fluoride) to be used twice daily after meals. Patient responded the oral therapy and soon got relieved of all the symptoms.
Surgical Treatment
All surgical procedure was planned under LA. A careful mucoperiosteal flap was raised with effect from the mesial aspect of 13 to th e distal aspect of 15. Careful removal of the surrounding bone was performed with the help of slow moving micromotor bur with continous saline irrigation and the supernumerary tooth was taken out and nanocrystalline CaSO4 hemihydrate bone graft was grafted in the bone defect to aid in healing and to maintain the natural bone contours and sutures were placed. Similarly inferior alveolar and lingual nerve blocks were given on the same side of the mouth, mucoperiosteal flap was raised and after judicial bone removal careful tooth extraction was done for both the extra teeth. Bone graft was grafted and sutures were placed. Similar procedure was performed on the right side of the jaw after 10 days of prior surgery. Sutures were removed on the 7th day post operatively and IOPA radiographs were taken to evaluate the bone morphology. Fig - 4, 5, 6, 7
 | Figure 4
|
 | Figure 5
|
 | Figure 6
|
 | Figure 7
|
Discussion
Multiple supernumerary teeth not associated with syndromes are a rare anomaly. Yusof in 1990 [6] reported that the premolar region in the lower arch is the most common place for supernumerary teeth followed by the molar region. Hegde and Munshi, Mason et al reported displacements, rotations, ectopic eruption, and malocclusion in their studies, similar alterations were noted in this clinical case. It is difficult to establish an ideal treatment for cases of multiple supernumeraries. The clinical and radiographic exam is of vital importance to carry out a good treatment plan which can vary from simple extractions or extractions followed by orthodontic treatment to obtain a correct occlusion. In this case it was decided to extract the erupted and retained supernumerary teeth followed by orthodontic treatment in order to establish a correct occlusion[8].We emphasize the importance of a good clinical history when a patient with multiple supernumerary teeth comes for consultation, since most of them are associated with other syndromes and their presence can be diagnosed by a routine dental professional, for example a patient of gardener's syndrome may manifest multiple osteomas of bone including skull and jaw bones and may also have multiple sebaceous or desmoids cysts on the scalp. In later life patient may manifest multiple polyposis intestine or carcinoma. Similarly a patient with cleidocranial dysplasia may manifest Delayed closure (ossification) of the bones of the skull (fontanels), Premature closing of the coronal suture , Protruding jaw (mandible) and protruding brow bone (frontal bossing) and wide nasal bridge due to increased space between the eyes (hypertelorism) Removal of supernumeraries should be evaluated for the possible benefits and for the treatment outcomes[9].Treatment depends on the type and position of the supernumerary tooth and on its effect or potential effect on adjacent teeth. The management of a supernumerary tooth should form part of a comprehensive treatment plan and should not be considered in isolation. Removal of the supernumerary tooth is recommended where: central incisor eruption has been delayed or inhibited; there is associated pathology; its presence would compromise secondary alveolar bone grafting in cleft lip and palate patients; the tooth is present in bone designated for implant placement and when the spontaneous eruption of the supernumerary has occurred.
Extraction is not always the treatment of choice for supernumerary teeth. They may be monitored without removal where: satisfactory eruption of related teeth has occurred; there is no associated pathology; removal would prejudice the vitality of the related teeth.
Removal of a supernumerary tooth preventing permanent tooth eruption usually results in the eruption of the tooth, provided adequate space is available in the arch to accommodate it.18 Di Biase found 75% of incisors erupted spontaneously after removal of the supernumerary. Eruption occurred on average within 18 months, provided that the incisor was not too far displaced and that sufficient space was available. Although the majority of authors recommend exposure of the unerupted tooth when the supernumerary is removed, Di Biase advocates conservative management without exposure [5].
Conclusions
Supernumeraries may be a result of biologic ,genetic and environmental factors[10]. Non syndrome associated supernumeraries is a rare entity and should be looked with a high suspicion of hidden syndrome and patient should be warned for future complications he may manifest. Supernumeraries that seem to be hazardous to the dentition should be removed carefully with proper maintenance of physiologic jaw contours .Impacted supernumerary teeth that are asymptomatic and do not affect the dentition should be followed rather than removed.
References
1. BS Suprabha, KN Sumanth,Karen Boaz, An unusual case of non syndromic occurance of multiple dental anomalies,Indian J Dent Res,20(3),2009
2. 1. Neville, Damn, Allen, Bouquot ,Oral and Maxillofacial pathology 5th edition -text book of oral pathology.
3. Shaffers, Heni,Levi. Textbook of oral pathology. 5th edition.
4. Dr. Sohinderjit singh ,Dr Prerna and Dr prikshit, Multiple supernumerary teeth- a case report:Indian J dent scien;2009:2:1,1-5
5. M. Garvey, Hugh J.Berry, Marielle Black, supernumerary teeth -An review of classification, diagnosis and management,J Can Dent Assoc 1999;65:612-6
6. Antonio Diaz, Jose Orozeo, Maria ,multiple hyperdontia:report of a case with 17 supernumerary teeth,Journal oral medicine and pathology:2008:E229-231
7. A Acikgoz, G Acikgoz, U Tunga ,characteristics and prevalence of non syndrome multiple supernumerary teeth;a case report, Dentomaxillofacial Radiology;2006:35,185-190
8. Pankaj Bansal, Sumidha Rastogi, archna agnihotri , Non -syndromic multiple impacted supernumerary teeth with peripheral giant cell granuloma,Contemp Clin Dent.2011 Jan -mar;2(1);41-44
9. Pavithra Shivastan, N Aravindha Bbu, mesiodens with an unusual morphology and multiple impacted supernumerary teeth in a non syndromic patient, Indian J dent Res 2007:18:3,138-14
10. Ullal anand Nayak , VM Mathian,Veerakumar,non syndrome associated multiple supernumerary teeth : A report of two cases,2006:24:5,11-14
|