Introduction
Trauma causes cessation of root development. Fragile root canals becomes weak. It is difficult to create an artificial barrier or induce closure of apical foramen with calcified tissue.[1]
MTA was first described in dental scientific literature in 1993[2] and was given approval for endodontic use by the US Food and Drug Administration in 1998. Upto 2002, only one MTA material consisting of grey coloured powder was available and then white MTA was introduced. Both formulae contain 75% Portland cement, 20% bismuth oxide and 5% gypsum by weight.
The aim of this procedure is to limit bacterial infection and production of mineralized apical tissues in immature anterior tooth.
The inadequacy of calcium hydroxide apexification due to its long time span and re-infection because of temporary seal[3],[4] led the use of MTA.
This forms a barrier and prevents micro leakage. It is bio- compatible and forms dentinal bridge, cementum and periodontal ligament regeneration.[5] It has the ability to stimulate cytocline release from the bone cells, indicating that it actively promotes hard tissue formation.[6]
Case Report
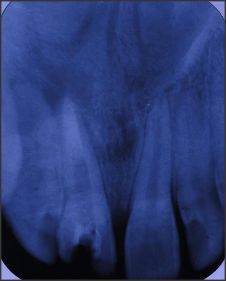
A 14 year old male presented with fractured maxillary right central incisor (Fig. 1). The patient reported of no tooth ache. The treatment of tooth was attempted by other dentist. Pulpectomy alongwith calcium hydroxide had been used as apical barrier for his last 6 months. But the treatment was not successful as seen in the radiograph (Fig. 2). The treatment involved was endodontic retreatment followed by esthetic enhancement by composite restoration of the tooth.
 | Figure 1
 |
 | Figure 2
|
Clinical Steps
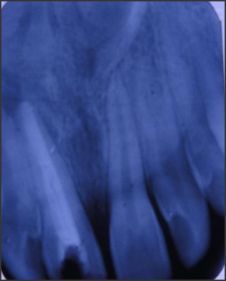
The tooth was isolated and access cavity re-negotiated. Canal was cleaned by endodontic files and 5% NaOCL and the length determined. The length was recorded for further refence. (Fig. 3).
 | Figure 3
|
The canal was dried with sterile paper points and once again calcium hydroxide dressing was given for 1 week by placing it with leutulo spirals (Dentsply Inc.).
After 1 week the calcium hydroxide was removed and rinsing of canal was done again with NaOcl and EDTA alternately. Finally after rinsing with sterile water canal was dried. MTA (Angelus, Londrina, PR, Brazil) was prepared according to manufacturer recommendation (Fig. 4). Mineral trioxide aggregate was placed in the apical portions of canals with a thickness of 3-5 mm. (Fig. 5).
 | Figure 4
|
 | Figure 5
|
A sterile moist cotton pellet was placed over the canal orifice and the access cavity was sealed temporarily.
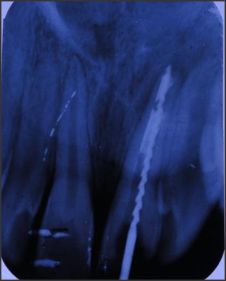
Correct placement was confirmed radiographically (Fig. 6). After one week the canal was filled with gulta percha points (Dentsply Tulsa) (Fig. 7). The esthetics of the fractured central incisor was restored with composite (shofu Inc. Japan) (Fig. 8).
 | Figure 6
|
 | Figure 7
|
 | Figure 8
|
Case was reviewed radiographically after an interval of 6 months (Fig. 9). The tooth was free of any visible or radiographic symptoms. Radiographically periapical tissue was normal and tooth was healthy.
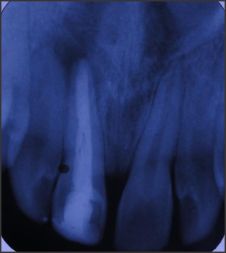 | Figure 9
|
Discussion
For many years the calcium hydroxide has been used in apexification in procedures. MTA is the material of choice which has been suggested with a choice which has been suggested with a repairing mechanism similar to calcium hydroxide but in a shorter period of time. It causes significantly less inflammation and also provides a hard-setting, non-resorbable surface without the presence of tunnels in the deutinal barrier.[7],[8],[9] Therefore in the case presented, MTA was used as material for apexification.
Many in vivo and hystological studies have reported the superior physical and biological properties of MTA in a short-folow-up period.[10],[11],[12]
Calcium hydroxide is unpredictable and have lengthy course of treatment and presents a challenge of re-infection as studied by Magura ME et al.[13]
Felippe WE et al.[14] & Regan JD[1] et al[15] used MTA as root end filling with promising results.
Conclusion
Long-term follow-up of MTA as not end filling shows good prognosis for immature fractured permanent teeth. One-step obstruction with MTA allows permanent restoration in a short time. Attempts are being conducted to improve the working properties of MTA via the addition of setting accelerators, shorter setting time, better handling properties and a similar sealing ability.
References
1. Seltzer S. Endodontology; Biologic Considerations in Endodontic Procedures, 1988, 2nd edn. Philadelphia; Lea and Febiger.
2. Lee SJ, Monset M, Torabinejad M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J. Endod 1993; 19 : 541-4.
3. Schmitt d, Bogen g. Multifaceted use of ProRoot MTA root canal repair material. Pediatr Dent 2001:23:326-30.
4. Andreasen JO, Farik B, Munksgaard BC. Long term calcium hydroxide as a root canal dressing can increase the risk of root canal fracture. Dental Traumatology 2002; 18 : 134-7.
5. Holah G, eidelman E, Fuks AB. Long-term evaluation of pulpotomy in primary molars using mineral trioxide aggregate or formocresol. Pediatr Dent 2005; 27:129-36.
6. Koh ET, Pittford TR, Torabinejad M, Mcdonald F. Mineral trioxide aggregate stimulates cytokine production in human osteoblasts J Bone Min Res 1995; 10S:S406.
7. Trope M, Chivian N, Sigurdsson A, Vann FV Jr. Traumatic injuries. In : Cohen S, Burns RC, editors, 8th ed., Pathways of the pulp. St. Louis, MO : Mosby; 2002, p. 603-49.
8. Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using mineral trioxide aggregate as a pulp capping material. J am Dent Assoc 1996; 127 : 1491-4.
9. Aeinechi M, Eslami B, Ghanbariha M, Saffar AS. Mineral trioxide aggregate and calcium hydroxide as pulp capping agents in human teeth: A preliminary report. Int. Endod J. 2003; 36 : 225-31.
10. Holland R, de Souza V, Murata SS, Nery MJ, Bernabe PF, Otoboni Filho JA, et al. Healing process of dog dental pulp after pulpotomy and pulp covering with mineral trioxide aggregate or Portland cement. Braz Dent J 2001; 12 : 109-13.
11. Khayat A, Abbasi A, Tanideh N. A comparative study of dentin bridge formation following pulpotomy using calcium hydroxide and mineral trioxide aggregate in young dogs. Ir J Vet res 2004; 5:47-54.
12. Karami B, Khayat A, Maozami F, Pardis S, Abott P. Histological evaluation of the effect of three medicaments : Trichloracetic acid, formocresol and mineral trioxide aggregate on pulpotomised teeth of dogs. Aust Endod J 2009; 35-18-28.
13. Magura ME, Kafrawy AH, Brown CE Jr. Netwon C. Human saliva coronal microleakage in obturated root canals; an in vitro study. Journal of Endodontics 1991, 17 : 324-31.
14. Felippe WT, Felippe Mcs, Rocha MJC. The effect of mineral trioxide aggregate on the apexification and periapical healing of teeth with incomplete root formation. International Endodontic Journal, 39, 2-3, 2006.
15. Regan JD, Guttman JL, Witherspoon DE Comparison Diaket and MTA when used as root end filling materials to support regeneration of periradicular tissues Int. Endod J 2002; 35 : 840-847. |