Introduction
Extrusive luxation or partial avulsion is the partial displacement of a tooth from its bony socket. Clinically the tooth appears elongated and mobile, and is most often displaced towards the palatal side[1]. Radiographically, an extruded tooth exhibits an increased periodontal ligament space after accident[2]. This type of dental injury is uncommon in the permanent dentition, and accounts for only 0.05 to 7% of all traumatized permanent teeth[2],[3]. Early treatment for dental extrusion (within 24 hours) is recommended in order to achieve optimal healing [4],[5]. The recommended treatment for dental extrusion is gentle repositioning and non-rigid splinting for 2 to 3 weeks[2],[6],[7]. This report describes the dental management of a girl with a traumatically extruded maxillary and mandibular incisors and multiple avulsion of maxillary teeth.
Case Report
An 8-year-old girl sought treatment for dental trauma in the Department of Paediatric and Preventive Dentistry that happened during the previous evening, about 18 hours prior to her presentation. She was treated at the Emergency ward of Government Medical Hospital immediately after trauma. The child gave history of fall from the first floor of a building while playing. Her medical history was unremarkable and all her vaccinations are up-to-date. There was no history of convulsions or vomiting and loss of consciousness. There was a positive history of bleeding from mouth and nose. Extra oral examination revealed swelling of upper and lower lips with tenderness on palpation; sutures were present on the lower lip. Intraoral examination revealed, avulsed 11, 21, 63 and 64. Tooth 22 was mobile, appeared elongated and displaced palatally. Teeth 31and 41 were also mobile and appeared elongated(Fig. I). Radiographic examination revealed coronal displacement of teeth 22,31and 41 (Fig. II). A diagnosis of extrusive luxation of 22, 31 and 41 was made. Under local anaesthesia, the mucosal wound was examined and no alveolar fracture was observed. Teeth 31 and 41 were then gently repositioned manually, and splinted to adjacent teeth with a 0.016-inch round stainless steel wire and composite resin. Tooth 22 was also gently repositioned manually, and splinted with suture splint as there was no tooth on either side of extruded 22 to support the splint (Fig. III). A cross suture with a nonresorbable silk suture material was placed over tooth 22 and the support was taken from the labial and palatal marginal gingiva. Light cure composite was cured over the suture material at the incisal third of the tooth so that the material does not slip. The sutures and splint were removed after one and two weeks respectively, and healing was uneventful (Fig. IV). The patient was reviewed after 6 weeks and 6 months and subsequently annually. All the traumatised incisors showed a positive response to the ethyl chloride test at all the review visits. Clinical and radiographic examination revealed satisfactory healing of the extruded incisors after 6 months (Fig. V).
 | Figure I; Preoperative photograph of the patient.
 |
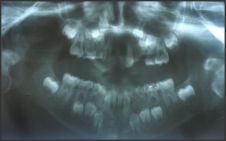 | Figure II; Preoperative radiograph showing avulsed 11,21,63,64 and extruded 22, 31 and 41.
|
![Figure III; Suture splint used for the stabilisation of repositioned 22.]](article-image-1697-FIGURE_III_SUTURE_SPLINT_USED_FOR_THE_STABILISATIO.jpg) | Figure III; Suture splint used for the stabilisation of repositioned 22.]
|
 | Figure IV; Postoperative radiograph of the patient.
|
 | Figure V; Postoperative photograph after six months (without removable partial denture for missing teeth).
|
Discussion
The prevalence of pulp necrosis following extrusive luxations was noted in two studies as 26 and 43%, respectively[8],[9]. Lee et al. Reported that pulp canal obliteration is the second most common healing complication following extrusive luxation injuries, as seen in 35% of the cases[9]. They reported that root resorptions are an uncommon outcome following extrusions. Andreasen and Vestergaard[9] found a significantly higher level of pulp necrosis in mature teeth; on the contrary, Lee et al.[9] noted the degree of extrusion as the main predictor for pulp necrosis as well as pulp canal obliteration after extrusions. The major factor influencing pulp healing after extrusive luxation was the stage of root development; immature teeth showed better healing potential compared with mature teeth[9]. In this case satisfactory healing was achieved in the traumatized incisors. The recommended treatment for dental extrusion is gentle repositioning and non-rigid splinting for 2 to 3 weeks[2],[6],[7]. Early treatment for traumatically extruded teeth is recommended, as delayed treatment might result in organization of the apical blood clot, making complete repositioning difficult[2], [4]. In this case the extruded teeth were repositioned with digital pressure on the same day. Fixation methods used for dental splints vary according to authors and with the type of dental trauma. Many different types of dental splints have been described in literature[9],[10],[11],[12]. Fixation after repositioning in case of mandibular central incisors was done with light cure composite and wire splint. This is one of the common methods of splinting opted for such kind of cases. But it was very difficult to stabilise the extruded maxillary central incisor after repositioning as teeth on either side of it were avulsed during trauma. Then it was decided to use suture splint[12] to stabilise this tooth. It is passive, semi rigid and functional splint[12]. It has been shown to be successful for stabilisation of such kind of injuries[13]. The splints were removed after two weeks. There was sufficient periodontal and gingival healing. Endodontic treatment, even for teeth with closed apices, should only be initiated when there is evidence of pulp necrosis or inflammatory root resorption[2]. The patient was reviewed after 6 weeks and 6 months and subsequently annually. All the traumatised incisors showed a positive response to the ethyl chloride test at all the review visits.
Conclusion
General dentists should familiarize themselves with the latest treatment protocols for dental trauma. A correct diagnosis and prompt treatment offers a better chance of optimal healing with fewer complications. Suture splints have been described, which are essential splints for the stabilisation of teeth under such conditions.
References
1. Andreason FM, Andreason JO. Extrusive luxation and lateral luxation. In: Andreason JO, Andreason L, editors. Textbook and color atlas of traumatic injuries to the teeth. 4th ed. Blackwell: Oxford;2007:411-27.
2. Subay RK, Kayatas M, Caniklioglu C. Delayed multipliscilinary management of extrusively luxated maxillary central incisor. Dent Traumatol 2007;23: 82-84.
3. Love RM, Ponnambalam Y. Dental and maxillofacial skeletal injuries seen at Otago School of Dentistry New Zealand 2000-2004. Dent Traumatol 2008;24:170-6.
4. Humphreys K, Al Badri S, Kinirons M, et al. Factors affecting outcomes of traumatically extruded permanent teeth in children.Pediatr Dent 2003;25:475-8.
5. Andreasen JO, Andreasen FM, Skeie A, Hjørting-Hansen E,Schwartz O. Effect of treatment delay upon pulp and periodontal healing of traumatic dental injuries-a review article. Dent Traumatol 2002;18:116-28.
6. Flores MT, Andreason L, Andreason LO, et al. Guidelines for the management of traumatic dental injuries. I Fractures and luxations of permanent teeth. Dent Traumatol 2007;23:66-71.
7. Kahler B, Heithersay GS. An evidence-based appraisal of splinting luxated, avulsed and root-fractured teeth. Dent Traumatol 2008;24: 2-10.
8. Andreason FM, Vestergaard PD. Prognosis of luxated permanent teeth: the development of pulp necrosis. Endod Dent Traumatol 1985;1:207-20.
9. Lee r, Baret EJ, Kenny DJ. Clinical outcomes for permanent incisor luxations in a pediatric population. II.Extrusions. Dent Traumatol 2003;19:274-9.
10. Oikarinen K. Tooth splinting: a review of the literature and consideration of the versatility of a wire-composite splint. Endod Dent Traumatol 1990;6:237-50.
11. Filippi A,B von Arx T, Lussi A. Comfort and discomfort of dental trauma splints- a comparison of new device(TTS) with three commonly used splinting techniques. Dent Traumatol 2002;18:275-80.
12. Gupta S, Sharma A, Dang N. Suture splint: an alternative for luxation injuries of teeth in pediatric patients-a case report. J Clin Pediatr Dent 1997;22:19-21.
13. Sheroan MM, Robert MW. Management of a complex dentoalveolar trauma with multiple avulsions: a case report. Dent Traumatol 2004;20:222-25.
|