Introduction
With the widening of horizons of surgical orthodontics, it has become apparent that neither surgery nor orthodontic tooth movement alone is sufficient for treatment of many patients. To obtain optimum results, a combination of surgery and orthodontic tooth movement is required in a majority of cases. The primary indication for a combined surgical-orthodontic treatment is the presence of severe malocclusion in an adult, whether it be largely a skeletal problem or primarily dental in origin. A careful evaluation of the diagnostic records should be done before planning treatment.[1] Close cooperation between orthodontist and oral surgeon is essential for proper treatment planning. Orthodontists must be aware of the variety of surgical procedures that are possible and about the relative difficulty and stability of each, and the surgeons must know the limits and possibility of orthodontic tooth movement. Both must aim towards the best occlusal and facial results possible for the patient.[2]
Anterior maxillary osteotomy is frequently applied to cases of maxillary excess. In addition to the anteroposterior problem, these cases are often accompanied with a long midfacial appearance and display of incisors and gingiva during smiling.To treat these patients, it is necessary to move the anterior maxillary segments upward as well as backward by anterior maxillary osteotomy. Anterior segmental osteotomies can be accomplished intraorally without any facial require and do not require prolonged intermaxillaryfixation.[4]
Case Report
A female patient aged 20yrs presented for treatmentto the Department of Orthodontics, Himachal Dental College, Sundernagar with a chief complaint of prominent upper front teeth and that her gums showed when she smiled.
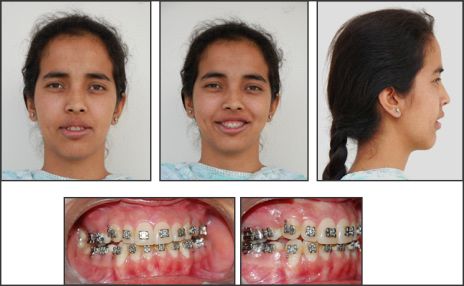
Dentofacial proportions and Esthetic evaluation : Onextraoral examination, no facial asymmetry was seen.Her profile demonstrated a marked protrusion of the maxilla.The frontal facial appearance showed a large vertical height and display of an entire incisor crown with a few millimeters ofgingiva on smile.There was lip incompetence and excessive exposure of upper front teeth.
Intraoral Examination : Intraoral examination revealed a Class II molar relation with increased overjet of 10mm. Crowding of anteriors was seen in lower arch.
Image 1 [Pre - Treatment]
 | Pre - Treatment
 |
Cephalometric Evaluation : Cephalometric examination revealed a moderately large ANB difference of 6o,a steep mandibular plane angle and proclined upper incisors. COGS analysis revealed increased anterior midfacial length, increased lower anterior facial height, increased posterior maxillary height, increased maxillary and mandibular dentoalveolar height and increased ramal length.
Model analysis : Examination of the models showed crowding in the lower arch with good arch symmetry and form in both upper and lower arch. Lower arch showed an increased curve of spee. A class II molar relation was present on both sides and increased overjet of 10mm was also seen.
The most significant problems were the protrusion and excessive vertical height of the maxilla. Therefore, the treatment plan was to move the anterior maxillary segment upward and backward by anterior maxillary osteotomy
Pre-Surgical Orthodontics:
A pre-adjusted edgewise appliance was placed and pre-surgical orthodontics was carried out with leveling and alignment of both arches and extraction of 1st premolars in lower arch to increase the overjet. Retraction of the anterior segment was done using sliding mechanics. Upper and lower arches were stabilized with 0.019 × 0.025" ss wire .The presurgical orthodontics was completed in 14 months.
Image 2 [Pre - Surgical Orthodontics]
 | Pre - Surgical Orthodontics
|
Surgical Treatment (Cupar technique)[5]
Patient underwent surgery under general anesthesia with nasotracheal intubation. Afterinfiltrating the mucosa with 2% lignocaine HCl with adrenaline 1: 80000 above the canines and premolars bilaterally, a vertical mucosal incision was made between canines and premolar from the gingival margin superiorly to the level of the anterior nasal floor, superior to root apex of the maxillary canine. The maxillary first premolars were extracted on both the sides.The measured amount of alveolar bone was removed and the osteotomy extended anteriorly to nasal aperture and same procedure performed on opposite side. A mucoperiosteal incision was made transversely across the palate just anterior to the ostectomysite.After the palatal bone was also removed, the anterior maxillary segment was down fractured and posterior and superior repositioning was done.The segments were immobilized with L-shaped miniplates.Suturing was done. No operative and postoperative complications were observed.
A decrease in maxillary dentoalveolar height and decrease in proclination of incisors was found postsurgically.
Image 3 - [Post - Surgical]
 | Post - Surgical
|
Post Surgical Orthodontics
Two months after surgery, a step was found between canine and premolars, so leveling and alignment was continued for correction of discrepancy.
Discussion
Although surgical procedures for treatment of Class III malocclusion has been an accepted treatment for many years, surgical procedures for correction of Class I and Class II malocclusion has gained tremendous interest in recent years. The major decision for correction of Class II malocclusion must be repositioning the maxilla distally or mandible forward. Treatment options for maxillary excess includes superior repositioning of the maxilla via total or segmental maxillary osteotomy , mandibular ramus osteotomy as a secondary procedure after maxilla is positioned vertically.[6] When the esthetic and functional requirements of the individual case can be satisfied by anterior maxillary surgery, this is the preferred operative approach since the surgical procedure is simple and the treatment results, including stability, are excellent.[7] The first report of an anterior segmental anterior maxillary osteotomy (ASMO) was published by Cohn-Stock in 1921.[8] After a transverse incision in the palatal mucosa, he made a wedge shaped ostectomypalatalto the anterior teeth. A greenstick fracture was then created at the ostectomy site, and the anterior maxilla was retracted. The anterior segment, however, relapsed within 4 weeks. Since then, the method has been developed and refined .The biologic process of healing of various modifications of this osteotomy has been studied in experimental models. Currently, mainly three variations of ASMO are used; the Wassmund, Wunderer,and downfracture methods. When the Wassmund[9] method is used, the anterior maxillary segment derives its blood supplyfrom both the facial and the palatal gingiva, as no flaps are raised. The planned osteotomy sites are reached by tunneling under the mucoperiosteum.
The Wunderer[10] method involves a palatal flap raised by means of a transverse incision of the palate. The anterior osteotomy is made after tunneling, leaving the buccal blood supply intact Is.
In the downfracture method, on the other hand, a buccal flap is raised, and the palatal osteotomy is made after tunneling, leaving the palatalblood supply intact.
The usual indications for ASMO are excessive vertical or anteroposterior development of the maxillary alveolar process in patients where the relationships between the posterior teeth are acceptable. When superior repositioning of the anterior part of the maxilla is the primary objective, the downfracture method is usually recommended, while the Wunderer method is more practical for posterior repositioning.
The main advantage of the Wassmund method is the excellent postoperative blood supply, and this technique is recommendedby some authors for all cases other than those requiring superiorrepositioning.
We corrected maxillary prognathism with anterior maxillary osteotomy (Cupar technique).No operative and postoperative complications were encountered.
References
1. Profitt WR, White RP.Treatment of severe malocclusions by correlated orthodontic-surgical procedures.Angle Orthod. 1970 Jan; 40(1):1-10.
2. Poulton DR. Surgical Orthodontics: Maxillary Procedures. Angle Orthod.1976; 46(4):312-331.
3. Suda N, Murakami C,Kawamoto T,Takeshima T,Fukada K, Harada K, Ohyama K.Three cases of anterior maxillary osteotomy under orotracheal intubation.Int J Adult OrthodOrthognathSurg 2002; 17:273-282.
4. Bell.W.H. Lefort 1 osteotomy for the correction of maxillary deformities. Journal of oral surgery 33:412; 1975.
5. Cupar I. Die ChirurgischeBehandlungder Form-turd Stellung-SveranderungenDes Oberkiefers, O&err. Z. Stomatol.51: 565, 1954; Bull. SC. Cons. Acad.R.P.F. Yougosl.2: 60, 1955.
6. Proffit WR, White RP, Sarver DM.Contemporary treatment of dentofacial deformity.
7. Jaj HS, MalhotraD,SinglaA,MahajanV,Jaj VP. Skeletal Open Bite Correction with Anterior Maxillary Osteotomy - A Case Report.Indian Journal of Dental Sciences. 2012 ;4(1):128-131.
8. Cohn-Stock G. DiecbirurgischeImmediatre - Gulierung der Kiefer, Speziell die chirurgische .Behandlung der Prognathie.VjschrZahnheilk Berlin 1921: 37: 320.
9. Wassmund, M. Lehrbueh de rpraktischenChirurgie des Mundcs under kicfer, Leipzig, 1935, Hermann Meusser, vol. 1.
10. Wunderer, S. Die Prognathie Operation Mittels Frontal GestieltemMaxillafeagment, Osterr. Z. Stomatol. 59: 98, 1962. |