Introduction
Heat polymerizing acrylic resin has been the most common denture base material. This material is preferred as denture base resin because of its physical and esthetic properties as well as the material availability, reasonable cost and ease of manipulation. However, the mechanical strength of polymethyl methaacrylate based denture base materials remain far from ideal for maintaining the longevity of dentures[1]. So the fracture of acrylic resin dentures is a common clinical occurrence. The strength of a denture depends on shape, residual stresses, and conditions of loading and mechanical properties of the material. Intrinsic strength of the material is affected by the composition which depends partly on the technique used. The principal factor in this respect is the amount of unpolymerised monomer remaining after curing. Fracture of repaired denture often occurs at the junction of an old and new material rather than through the center of the repair.
Regardless of the reason for fracture or the method for repair, the ultimate goal of denture repair is to restore original strength of the denture and to avoid further fracture. The repair of the fractured prosthesis can be accomplished using acrylic resins that are heat polymerized, auto polymerized or light polymerized. Out of these the repair strength of heat polymerized resin is highest and ranges from 75-80% of the original material[2]. Various joint interface contours as butt, rounded and 45 degree bevel joint designs have also been found to influence strength of the repairing unit [3],[4].
Mechanical modifications improve the bond strength by increasing the surface area and mechanical retention.[5] Organic solvents such as ethyl acetate, methylene chloride, chloroform causes etching of the surface of denture base resins and increases mechanical interlocking thereby significantly improving the bond strength between acrylic denture base and repair resin.[6]
Methodology
Preparation of Test Samples
Test samples of heat cure acrylic resin (Trevalon H1) of dimensions 60mm x 4mm x 6mm were prepared. The metal blocks were coated with petroleum jelly and invested in dental flasks. After the setting of the Plaster Of Paris, the flasks were opened and the metal blocks were removed. These formed plaster moulds in the flasks. Cold mold seal was applied. Heat cure acrylic resin ( Trevalon HI) was mixed and packed in these plaster moulds. Then processing was done in a water bath at a temperature of 74 C for approximately 2 hours and then the temperature of the water bath was increased to 1000C and processing was continued for another hour. After curing the samples were removed and finished.
These samples were divided into six groups of 10 specimens each.
1. Specimens were repaired with heat cure acrylic resin.
2. Specimens were chemically treated with ethylacetate and repaired with heat cure acrylic resin.
3. Specimens were repaired with self cure acrylic resin.
4. Specimens were chemically treated with ethylacetate and repaired with self cure acrylic resin.
5. Edges of specimens were made rounded before repairing with self cure acrylic resin.
6. The edges of cut specimens were made at 450 beveled before repairing with self cure acrylic resin.
Preparation Of Repair Indices
For preparing repair indices larger sized (65mm x 4mm x 6mm) metal blocks were used so as to leave a gap of 5mm for the repair material. After coating the metal blocks with petroleum jelly, these blocks were invested in denture flasks. After the plaster was set, the metal blocks were carefully removed from the working plaster mould. Acrylic specimens were cut in the centre to form 2 parts of 30 mm length.
Repair with heat cure acrylic resin: The two halves of acrylic specimens were placed on both sides of the repair index with a gap of 5 mm between them. The two surfaces facing each other were made rough with a bur. Heat cure resin was mixed in a clean container and in the dough stage it was packed in the gap between the two specimens. The repaired specimen was cured at 740C for 2 hours and then at 1000C for 1 hour.
Repair with heat cure acrylic resin after Chemical Treatment: The two halves were treated with ethylacetate. One face each of both specimens was dipped in ethyl acetate liquid for 60 seconds and then dried. Then these specimens were placed in the repair index with the treated edges faces each other and repaired with heat cure resin.
Repair with self cure acrylic resin: The two halves were placed in the repair index with a gap of 5mm in between. Now the self cure acrylic resin was mixed in a clear container and packed in the gap between the specimens. Then the self cure resin was allowed to cure.
Repair with Self cure acrylic resin with chemical treatment: The two halves were treated with ethylaetate. One face each of both specimens was dipped in ethyl acetate liquid for 60 seconds and then dried. The specimens were then placed in repair index with treated edges facing each other and repaired with self cure resin.
Repair with self cure resin with 45o bevel edges: In this one face each of both halves was made beveled at 45o with the help of a carbide bur. Then the halves with the 45o bevel face facing each other were placed in the repair index and repair was done with self cure resin.
Repair with Self cure resin with round edges: One face of both halves was made rounded with the help of a carbide bur. Then halves with the rounded face facing each other were placed in the repair index and repaired with self cure resin.
Testing of Repaired specimens
All repaired specimens were tested for transverse strength in an Instron Universal Testing Machine. For testing, the specimens were placed between the two holding clamps of Universal Testing Machine & locked. Now the tensile load was set to zero and increased progressively until the specimen was broken. The reading in machine was noted. (Using the main and vernier scale)
Statistical Analysis
Statistical analysis was done with standard computer software. One way ANOVA TEST (p 0.05) was used to determine the differences between the individual groups.
Results
Group 1 specimens repaired with heat cure acrylic resin, range of transverse strength is 67.30-69.50 kg and mean is 68.53 kg.
Group 2 specimens repaired with heat cure acrylic resin after chemical treatment, range is 73.20-75.60 kg and mean is 74.18 kg.
Group 3 specimens repaired with self cure acrylic resin, range is 36.40-38.10 kg and mean is 37.3 kg.
Group 4 specimens repaired with self cure acrylic resin after chemical treatment, range is 42.10-44.00 kg and mean is 43.12 kg.
Group 5 specimens repaired with self cure acrylic resin with rounded joint surface contour, range is 54.30-56.00 kg and mean is 54.97 kg.
Group 6 specimens repaired with self cure acrylic resin with 45 degree joint surface contour, range is 50.20-52.10 kg and mean is 51.23 kg.
Statistical Results
One way ANOVA TEST (p 0.05) with standard error of 0.31207 showed that mean difference between all possible paired combinations among the six groups were statistically highly significant Group2 having specimens repaired with heat cure acrylic resin after chemical treatment exhibited highest transverse strength.
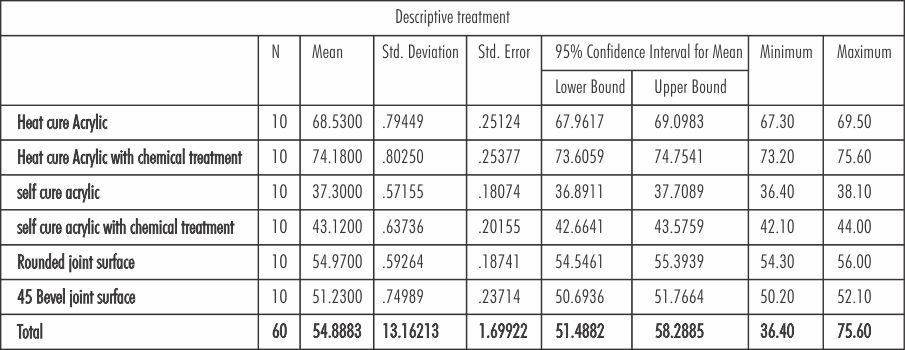 | Table Showing Mean And Standard Deviation Values Of Tranverse Strength Of Repaired Specimens
 |
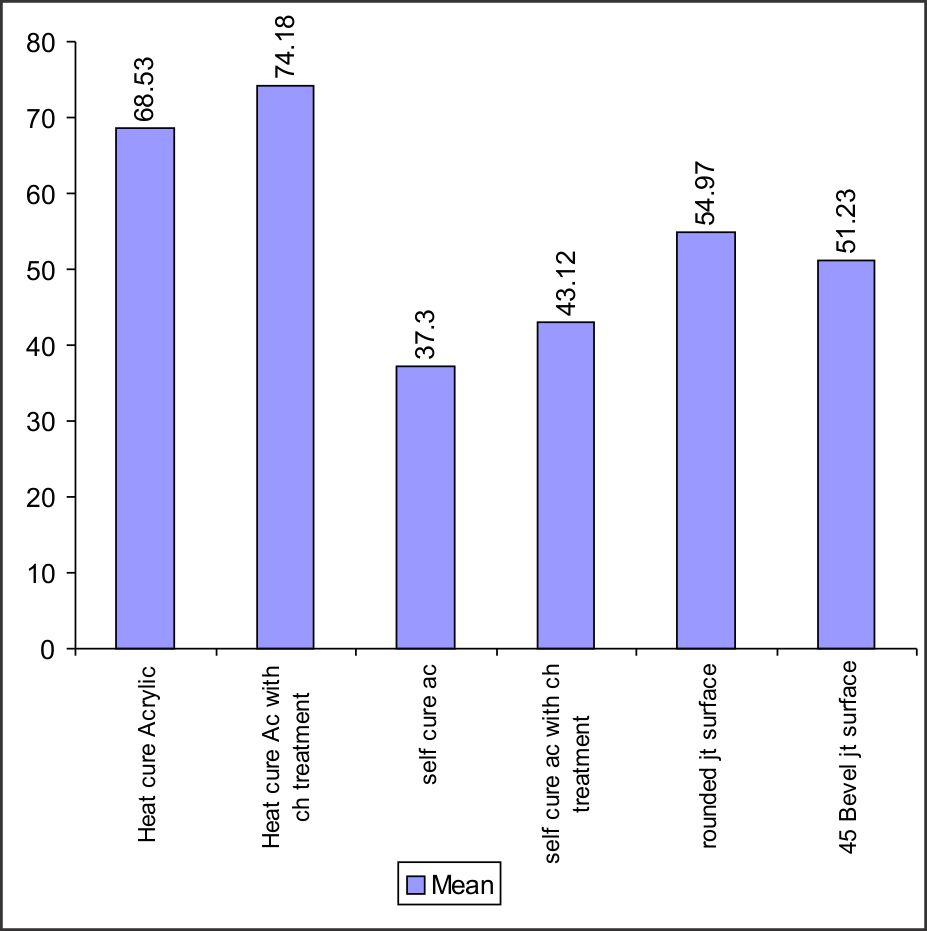 | Bar Diagram Showing Mean And Standard Deviation Values Of Tranverse Strength Of Repaired Specimens
|
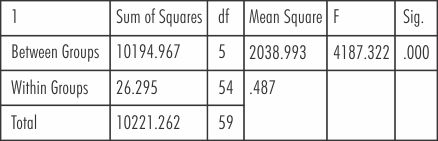 | ANOVA Treatment
|
Discussion
The fracture of acrylic dentures is a long standing problem and a common clinical occurrence. Denture fracture is usually due to faulty design, fabrication and material choice in prosthodontic practice. The repair of the fractured prosthesis can be accomplished using acrylic resins that are heat polymerized auto polymerized or light polymerized. Various joint interface contours as butt, rounded and 45 degree bevel joint designs have also been found to influence strength of the repairing unit. Several authors suggested chemical surface modifications using organic solvents as ethyl acetate, methylene chloride and chloroform to improve the bond strength of a repair material to denture base.[6],[7]
The purpose of the present study was to compare the effect of repair material, surface design and
chemical treatment on the transverse strength of repaired acrylic denture base.
60 test samples of heat sure acrylic resin (Trevalon HI) were repaired with Heat cure acrylic resin, Heat cure acrylic resin with chemical treatment, Self cure acrylic resin, Self cure acrylic resin with chemical treatment, Self cure acrylic resin with 450 bevel joint surface contours and Self cure acrylic resin with rounded joint surface contours
The results of this study demonstrated that transverse strength of specimens repaired with heat cured acrylic resin (68.53 kg ± 0.79) was higher than that of self cure acrylic resin (37.3 kg ± 0.57), self cure acrylic resin with chemical treatment (43.12 ± 0.63), with 450 bevel joint surface contour (51.23kg ± 0.74) and with rounded joint surface contour (54.97 kg ± 0.59).
The present study demonstrated higher transverse strength value of 68.53 kg ± 0.79 for heat polymerized resin and 37.2 kg ± 0.57 for self cure resins. These results were in agreement with the studies done by Skinners EW (1954),[8] Carl HJ and Sweeny WT (1955),[9] Anderson (1958), Beyli MS et al (1980),[10] Stanford JW (1989).[11]
The greater values of bond strength of heat cured resins over self cured resins as repair materials can be attributed to higher degree of polymerization and lower residual monomer content of heat polymerized resin (Skinner EW, 1954).[8]
Attempts to improve the bond strength of repair material to denture base resins by means of chemical treatment of repair surfaces were advocated by several investigators. It had been reported by Skinner EW (1954)[8] that such surface treatment caused superficial crack propagation as well as formation of numerous pits approximately 2 mm in diameter. Etching the repair surface with chemical etchants as chloroform, acetone, methylmethaacrylate , methylene chloride, ethylacetate was suggested by various investigators. In the present study maximum transverse strength (74.18+0.28) was observed with repair using heat cure acrylic resin after chemical treatment of broken edges with ethylacetate.
The transverse strength of repair with self cure resin with chemical treatment was greater (43.12 ± 0.63) than that of repair with self cure resin (37.3 ± 0.57) without chemical modification of repair surfaces. However it was less than that of repair with heat cured acrylic resin with chemical treatment (74.18 ± 0.28).
Nagai E et al (2001)[12] evaluated the strength and modulus of elasticity of repaired acrylic resin specimen reinforced with various processes and observed that surface pretreatment with methylene chloride created tight adhesion of auto polymerizing and heat polymerizing resin.
Ward JE et al (1992)[4] reported that the surface design that provides the greatest strength would decrease the number of adhesive failures.
To assess the effect of type of repair joint on the strength of repaired acrylic denture base, edges of the specimen instead of making butt joint were (i) rounded and (ii) contoured to 450 bevels before repairing with self cure acrylic resin. It was observed that strengths of repair made by self cure resin with round joint surface contours (54.97 ±0.59) and 450 bevel joint surface contour (51.23 ± 0.74) was greater than the repair with chemical treatment (48.12 ± 0.63). The transverse bond strength of 450 bevels joint was slightly higher than rounded joint but the differences were not statistically significant. However the repair strength of butt joint (37.3 ± 0.571) was significantly less than that of rounded or 450 bevel joint.
The results of this study are in accordance with previous studies by Harrison WM and Stausbury BE (1970),[3] Beyli K (1980) and Ward JE (1991).[4] Improved transverse strength of repair with round and 450 bevel joint designs is due to greater area of contact between repair and base material than repair with butt joint.
The fact that the rounded joint is superior to butt joint support the general principal that sharp angled surface promote stress concentration and that the amount of stress concentration is directly related to the degree and abruptness of surface change. Therefore, since residual stress is produced and sharp angled surface concentrate the stresses when repairing fractured acrylic resin prosthesis, one should attempt to prevent recurrent structural fracture by distributing these stresses as evenly as possible by preparing a joint with rounded interface.
According to the results obtained in this study, transverse strength of repaired acrylic denture base was highest when repair was done using heat cure acrylic resin, particularly after chemical treatment with ethyl acetate. The study also exhibited that repair joint surface configuration influences the transverse strength of repair material. Rounded and 450 bevel joint contours had significantly improved repair strength than repair with butt joint.
At present no repair material meets the ideal requisites as optimal transverse strength, ease of manipulation, cost and inconspicuousness. As fabrication of new denture is an expensive and time consuming procedure, clinical knowledge about the choice of material and method of repair is important till a definite prosthesis can be fabricated for the patient.
Although this in vitro study evaluated the effect of repair material, surface design and chemical treatment on transverse strength of repaired acrylic denture base, it did not simulate the clinical condition, ideally, as repaired dentures are exposed to repeated mechanical stresses during mastication. Also the use of a simple rectangular shaped specimen rather than a complex denture design contributes to the limitations of the present study. Therefore further investigations are necessary to evaluate the strength of repair under more closely simulated clinical conditions.
Summary and Conclusion
Within the limits of the study, it can be concluded that choice of material and method of repair have significant effect on strength of repaired denture .Chemical treatment prior to repair with heat cure acrylic resin as well as rounded and 45 degree beveled joints enhance the bond strength of repair material.
References
1. Seo RS, Murata H, Hong G, Vergani CE and Hamada T: Influence of thermal and mechanical stress on the strength of intact and relined denture bases. J Prosthet Dent 2006, 96; 59-67.
2. Rached RN, Powers JM and Del Bel Cury AA: Repair strength of autopolymerising microwave, and conventional heat-polymerized acrylic resins. J Prosthet Dent 2004; 92:79-82.
3. Harrison WM and Stansbury BE. The effect of joint surface contours on the transverse strength of repaired acrylic resin. J Prosthet Dent 1970; 23: 464-71.
4. Ward JE, Moon PC, Levine RA and Behrendt CL : Effect of repair surface design, repair material, and processing method on the transverse strength of repaired acrylic denture resin. J Prosthet Dent 1992; 67:815-820.
5. Minami H, Suzuki S, Minesaki Y, Kurashige H and Tanaka T. In vitro evaluation of the influence of repairing condition of denture base resin on the bonding of autopolymerising rsins. J Prosthet Dent 2004; 91: 164-70.
6. Sarac YS, Sarac D, Kulunk T and Kulunk S: The effect of chemical surface treatments of different denture base resins on the shear bond strength of denture repair. J Prosthet Dent 2005 94:256-66.
7. Vallittu PK, Lassila VP and Lappalainen R : Wetting the repair surfec with methyl methacryylate affects the transverse strength of repaired heart-polymerized resin J Prosthet Dent 1994; 72: 639-42
8. Skinner EW (1954). Quoted by McCrorie JW and Anderson JN. Transverse strength of repairs with self curing resins. British Dent Journal 1960; 109: 364-66.
9. Caul HJ and Sweeny WT (1955). Quoted by McCrorie JW and Anderson JN. Transverse strength of repairs with self curing resins. British Dent Journal 1960; 109: 364-66.
10. Beyli MS and Von Fraunhofer JA. Repair of fractured acrylic resin J Prosthet Dent 1980; 44:497-502.
11. Stanford JW, Burns CL and Paffenbarger GC : Self - curing resins for repairing dentures: some physical properties J Prosthet Dent 1989; 51: 307-15.
12. Nagai E, Otani K, Satosh Y and Suzuki S. Repair of denture base resin using woven metal and glass fiber: Effect of methylene chloride pretreatment. J Prosthet Dent 2001; 85: 496-500.
13. Smith DC: The Acrylic Denture- Mechanical evaluation of mid-line fracture. British Dental Journal 1961; 110: 257-67.
14. Stafford GD and Smith DC: Flexural fatigue tests of some denture base polymers. British dental journal 1970; 128: 442-445.
15. Stipho HD, Talic YF: Repair of denture base resins with light polymerized reline material: Effect on tensile and shear bond strengths J Prosthet Dent 2001 Vol. 86: 143-48. |