Introduction
The three dimensional obturation of the root canal system is widely accepted as a key factor for successful endodontic therapy. Its success is dependent on excellence of endodontic design and thorough cleaning and shaping. The aim of endodontic treatment is to fill the entire root canal system and all its complex anatomic pathways completely and densely with non-irritating hermetic sealing agents to prevent re-infection and percolation of bacterial substrates, which could cause biological breakdown of attachment apparatus[1],[2].Total obliteration of the canal space and perfect sealing of the apical foramen at the dentin cementum junction and accessory canals at locations other than the root apex with an inert, dimensionally stable, and biological compatible material are the goals of successful endodontic treatment[3].
Nearly 60% of endodontic failures are apparently caused by incomplete obliteration of the canal space.[4] Unless, a dense, well adapted root canal filling is achieved, the prognosis may be compromised regardless of how other phases of the treatment are carried out. Seltzer noted that metabolites are exchanged on a permanent basis between the root canal and the saliva.[5] Naidorf indicated that improper obturation can allow fluids to enter the root canal space which as a result may become infected.[6],[7] Over many years, different obturating materials, techniques and endodontic sealers have been introduced in a hope to increase the quality of apical seal.
A wide range of root canal materials have been used from time to time. Guttapercha introduced by Bowman in 1867 is the most widely used and accepted root canal filling material. It exists in various phases such as alpha, beta & gamma phase, which are interchangeable. Taking advantage of the phase changes of guttapercha and the resultant differences in physical properties recent developments have dealt with heating or thermoplasticizing the material to 420C temperature or even higher. The delivery system employed for thermoplasticized guttapercha is, heating it by electricity or a rotating instrument, resulting in a single mass. The softened material is then distributed into the canal often with an injection tip to develop homogeneity which in turn results in reduction of voids.[4],[7] As handling thermoplasticized guttapercha requires lot of skill, often canals were overfilled by inexperienced operators. Maintenance of uniform temperature during obturation is also quite difficult.
In recent years a silicon based sealer, Roeko Seal Automix was introduced which has shown to provide a hermetic seal over a period of 18 months.[8] An innovative root canal paste named Gutta Flow is developed recently which is a modification over RoekoSeal. It has an improved seal and better adaptability to the root canal wall because of the increased flowability and expansion on setting.[9]
Gutta Flow is a cold flowable guttapercha filling system for the obturation of root canals. It is composed of a polydimethylsiloxane matrix incorporating sealer and very finely ground guttapercha in one product. It has extraordinary chemical and physical properties that offer maximum sealing ability and biocompatibility. It does not shrink but expands slightly on setting when inserted in the root canal resulting in an excellent seal. It also has a superior flow which allows for optimal distribution of the material throughout the root canal. The material is thixotropic its viscosity diminishes under pressure thus allowing it to flow into the smallest of lateral as well as accessory canals. This new root canal obturation material was developed to overcome the shortcomings of lateral condensation technique.
With the above background the present study was designed to compare the adaptability of Gutta Flow paste and conventional laterally condensed guttapercha using AH-plus as a sealer, to the root canal walls using a stereo zoom microscope.
Materials & Methods
This ex-vivo study was conducted in the Department of Conservative Dentistry and Endodontics at Saraswati Dental College and Hospital, Lucknow, India and further work regarding stereozoommicroscopic procedures and observations were carried out at Division of Toxicology, Central Drug Research Institute (CDRI), Lucknow, India. For the purpose of study, 120 single rooted extracted human premolar teeth with intact crown were selected. After visual examination, surface deposits and soft tissue attachment were removed with an ultrasonic scaler. All the teeth were stored in 5.25% sodium hypochlorite solution (Prime Dental Products, India) for 48 hours to eliminate remaining organic debris. The teeth were washed under tap water and stored in normal saline.
Access Cavity Preparation
After measuring the shape, size and the extension of the pulp chamber radiographically, access was gained through the occlusal surface. No. 2 round bur in a high speed contra-angle hand piece was used to open the pulp chamber the bur felt to “drop” when the pulp chamber was reached. While removing the bur, the orifice was widened buccolingually in an ovoid shape. Buccolingual extension and finish of cavity wall was done with a 701 U fissure bur at high speed. Final preparation provided unhindered access to canal orifices which was made extensive enough to allow for instruments and filling materials needed to enlarge and fill canals.
Estimation Of Working Length
A#10 K file (Mani, Japan) was introduced into canal until the tip was just visible at the apical foramen. The working length was determined by subtracting 1 mm from this length.
Biomechanical Preparation Of The Specimens
Using a step back technique, the canals were cleaned, shaped & enlarged with K files (Mani, Japan) to the working length at the apex, initially they were prepared by # 10 K file (Mani, Japan) followed by sizes 15, 20, 25 & 30 and preflaring was carried out with Protapers (Dentsply Co. U.S.A.) at 300 rpm with a torque control micro motor having a preprogrammed setting (X-Smart, Dentsply USA). RC prep (Premier Dental Co. USA) was used along with the Protaper NiTi rotary instruments for adequate lubrication, cleaning and shaping. Frequent recapitulation and copious irrigation with 5.25 % Sodium Hypochlorite solution was carried out before progressing to next instrument, final preparation was done till # 50 file.
After biomechanical preparation, all the specimens were thoroughly irrigated with 17 % EDTA, 10 ml of 5.25 % Sodium Hypochloride (NaOCl) and finally with 10 ml of normal saline. The irrigating solutions were delivered from a 26-gauge needle which was made blunt at the tip. At this stage, 120 teeth were divided into four groups using stratified randomization. All the teeth were stored in normal saline until obturation to simulate oral environmental conditions.
Obturation
Group A (Control) consisted of 30 teeth that were obturated with Lateral condensation technique using AH plus as a sealer. (Fig-1) Group B (Experimental) consisted of the remaining 90 teeth. This group was further sub divided into three subgroups consisting of 30 teeth each.
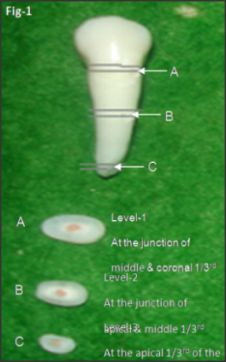 | Fig-1 : Sectioning levels
 |
These subgroups were:
B1 Obturation was done only with Gutta flow. (Fig-2)
B2 One guttapercha cone was introduced in the canal and the obturation was carried out similar to as B1 sub group. (Fig-3)
B3 Two guttapercha cones were introduced in the canal and the obturation was carried out in the similar manner as B1 subgroup. (Fig-4)
Sectioning Of Teeth And Observations
After obturation the roots were sectioned transversally. Sectioning of the teeth was not performed at a predetermined distance from the apex (because sectioning at a predetermined distance from the apex does not give information about the position of the sectioning levels in relation to coronal access cavity), but rather according to the individual root length. This was done to obtain comparable information regarding obturation at specific root level for e.g. Obturating a root canal at a level 5mm short of the apex may be easier to perform in short root canals than in long ones.
 | Fig-2 : GROUP-A (laterally condensed GP with AH plus)
|
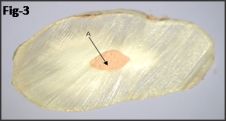 | Fig-3 : SUB GROUP - B1 A-Obturation with only Gutta Flow
|
 | Fig-4 : SUB GROUP - B2 A-Obturation with Gutta Flow and B - single GP
|
The thickness of the sections was 1 to 2mm. Sectioning was carried out using a Diamond saw (Cir-Saw, Confident Dental Co., India) at slow speed with constant water cooling to avoid excess heat generation which could result in softening of guttapercha point and also can cause its extrusion from root canal.
Level 1 : At the apical 1/3rd of the root 1mm from the apex as fins and narrow oval canals are very common in these regions which are difficult to prepare, irrigants do penetrate easily and obturation is difficult.
Level 2 : At the junction of the middle and coronal 1/3rd. Because at the coronal part of the canal, adaptation of the filling material is easier as there is ease of accessibility and preflaring of the root canal.
Level 3 : At the middle and coronal 1/3rd (Fig-5)
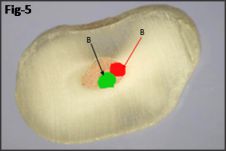 | Fig-5 : SUB GROUP - B3 Obturation with Gutta Flow and B -two GP points
|
These sections were observed and measured using a Stereomicroscope with zooming facility for the number of voids in Periphery & Core. These observations were subsequently labeled, digitally photographed and voids were measured using Biovis Image Plus (Software for image analysis and processing), Exper Vision Labs Pvt. Ltd, Mumbai, India. The data so collected were statistically analyzed using one way ANOVA followed with Tukey's test.
Result
The findings and observations on this study have been summarized hereunder and wherever deemed necessary, it has been presented in the form of figures and illustrations (Table -1 & Fig. 1 to 6). The area of voids were found to be insignificant when subgroup B1 was compared with group A and subgroup B2 (P>0.05), where as a significant number of voids have been observed in sub group B3 when it was compared to other sub groups and group A (P<0.01). The variance of all the four groups was found to be homogeneous.
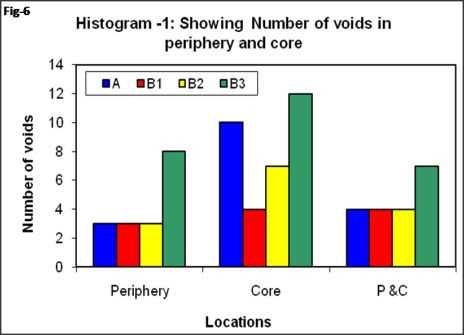 | Fig-6 : Histogram showing number of voids on periphery and core.
|
 | Table 1: Comparison of cephalometric variables for Canine guided and Group function occlusion (overall) (n=60)
|
Numbers of voids in locations of four groups were shown graphically. Locations wise B1 showed the least number of voids (4 in core & 3 at the periphery) whereas B3 demonstrated maximum number of voids (12 in core & 8 at the periphery). A highest percentage of number of voids could be noted among the teeth of subgroup B3 (47.1%in core and 36.4% at the periphery) while B1 show the least number of voids (17.6 %in core and 12.1% at the periphery). The lowest mean of area of voids was recorded statistically in the Gutta Flow subgroup, which was obturated without using any gutta percha.
Statistically there was no difference in the area of voids in Gutta Flow subgroup using a single cone when compared with the conventional lateral condensation group using AH plus as a sealer. The highest frequency of sections with voids was observed in Gutta Flow subgroup in which obturation was done utilizing two cones. It was statistically significant when compared to the other groups.
When the sectioning levels were separately analyzed the sections made at the middle 1/3rd showed the maximum number of voids among all the groups. The maximum numbers of voids were located at the core of the filling. The sizes of individual voids in all the groups were statistically insignificant except in the Gutta Flow group having two cones.
Discussion
Three-dimensional ‘fluid tight’ obturation and a well-fitting ‘leakage-free’ coronal restoration prevent percolation and micro leakage of periapical exudate into the root canal space thus reducing the chances of re-infection. It also creates a favorable biological environment for tissue healing to take place.[10]
Incomplete root canal obturation has generally been considered as one of the principal cause of endodontic failure.[11] In the past various materials and techniques were tried to obtain a hermetic seal. The sealing ability & adaptability of various root canal filling materials were studied over the years and it was found that none of the available materials satisfactorily provide a hermetic seal.[12] Because of the above reason currently used techniques utilize several materials for obturation, the most common being a combination of guttapercha and sealer. Numerous techniques have been developed to improve adaptation of the sealer to the root canal walls and to reduce its film thickness to minimum.[13]
This ex-vivo study was undertaken to comparatively evaluate the adaptability of cold flowable gutta-percha paste i.e. Gutta Flow and conventional laterally condensed guttapercha using AH-Plus as a sealer, to the root canal walls. Gutta-flow was compared to conventional lateral condensation, because this technique is believed to be the gold standard for obturation. Selection of the teeth and their assignment into different study groups was done using stratified and block randomization, which resulted in comparable groups with respect to tooth type and form. (Long/short and straight/curved).
In the present study only extracted single rooted (premolar) human teeth having intact crowns were considered, so as to simulate the clinical conditions because decoronation of teeth can result in easy accessibility to root canals[14]. The root canal sealer used was AH plus with prefabricated, standardized guttapercha cones. Cold lateral condensation technique was used for Obturation as for years lateral condensation of guttapercha has been a benchmark for obturation. This technique has been credited to Callahan in 1914[15] and the technical details of application were provided by Sommer in 1946.[16] The effectiveness in obtaining three dimensional (3D) seal was confirmed by the studies of Marshall and Massler[17] and Weine.[18] However, this technique still remains the gold standard and most of the studies utilizing new obturation systems use lateral condensation for comparison purposes.[19]
Stereomicroscopic examination was chosen for this study, as it gives a 3-D view of the surface to be examined, needs no pretreatment of the specimen (as in SEM Examination). The area of voids was calculated utilizing Software for Image Analysis (Biovis Image Plus) thus eliminating human error in interpretation of the data.
Based on the results of this study, the first and the second sub group i.e. Gutta Flow obturation without guttapercha and with a single cone guttapercha showed a lesser number of voids in the sections as compared to the one obturated with two cones respectively. Nearly all the voids in this group were found mainly in the core or between the core and periphery. The minute voids in the core can be either because of using lentulo spiral or due to manufacturing process. On the other hand when obturation was done using two cones the number and size of voids was comparatively larger and was present in all regions of the root canal it can be due to entrapment of air when second guttapercha point is inserted or because of absence of lateral condensation. Among all the sub groups negligible voids were found at the periphery of the root canal wall, suggesting that the adaptation of the material to the walls was nearly complete. This can be attributed to the property of Gutta Flow which does not shrink but expands slightly (0.2%) on setting resulting in an excellent seal of the root canal.
In Group B the number and the size of voids were statistically insignificant when compared to Group A. The minute voids observed can be due to difficulty in lateral condensation of the curved canals. The walls of the root canal showed good adaptation of AH-plus sealer.
Number of voids was ascertained by examining the periphery or core of the root canal. Locations wise B1 showed the least number of voids (4 in core & 3 at the periphery) whereas B3 demonstrated maximum number of voids (12 in core & 8 at the periphery).
A highest percentage of number of voids could be noted among the teeth of subgroup B3 (47.1%in core and 36.4% at the periphery) whereas B1 show the least number of voids (17.6 %in core and 12.1% at the periphery) which is again in conformity with the above findings.
Gutta Flow group, which was obturated without using any guttapercha cone and obturation utilizing a single cone showed no difference in the area of voids statistically when compared to the conventional lateral condensation group using AH plus as a sealer. The highest frequency of voids was observed in Gutta Flow group in which obturation was done utilizing two cones. It was statistically significantly higher when compared to other groups.
When the sectioning levels were separately analyzed the sections made at the middle showed the maximum number of voids in all the groups. The maximum numbers of voids were located at the core of the filling. The sizes of individual voids in all the groups were statistically insignificant except in the Gutta Flow group having two cones.
Conclusion
Based on the results shown, the following conclusions were drawn from the study
1. The Gutta Flow sub group without gutta-percha & with single cone guttapercha showed minute and lesser number of voids and better adaptation to the root canal walls.
2. There was presence of small voids within the core of the material in all the groups.
3. Gutta Flow uniformly adapted to the root canal walls.
In the light of the above results and paucity of literature, it is apparent that this approach is use full for the purpose however, further study is called for to substantiate the view.
References:
1. Davalou S, Gutmann J. L, Nunn M. H. (1999) Assessment of apical and coronal root canal seals using contemporary endodontic obturation and restorative materials and techniques. International Endodontics Journal 32,388-396.
2. Kakeshashi S, Stanley HR, Fitzgerald RJ. (1965) The effects of surgical exposures of dental pulps in germ free and conventional laboratory rats. Oral Medicine and Oral Pathology 20, 340-9.
3. Grove C.J. (1931) Why Root canal should be filled to the Dentino- cemental junction. Journal of American Dental Association 19,314.
4. John and Leif (2002). John I. Ingle, Leif K.Bakland. Textbook of Endodontics. Obturation of radicular space .5th edi 2002: 598-636.
5. Seltzer S. (1988) Root canal fillings in Endodontology Biologic considerations in Endodontic Procedures, 2ndedi, 357-78.
6. Naidorf IJ. (1974) Clinical microbiology in endodontics. DCNA 18,329.
7. Combe E.C., Cohen B.D., Cummings K . (2001) ? & ß forms of guttapercha in products for root canal filling. International Endodo Journal 34,447-451.
8. Wu MK, Tigos E, Wesselink PR. (2002) An 18-month longitudinal study on a new silicon based sealer RSA Roeko Seal: A leakage study in vitro.Oral Surgery Oral Medicine Oral Pathology Oral Radiology and Endodontics 94, 499-502.
9. PommerO,.Neumann U, Attin T. (2001) In vitro evaluation of dye leakage of a new siloxane-based root canal sealer. International Endodontics Journal 86,11.
10. Nguyen NT, Cohen S Burns. (1994). Pathways of the pulp, Obturation of the root canal system 6thedition, 219-271.
11. Dow P.R, Ingle J.I. (1955) Isotope determination of root canal failure. Oral Surgery 8,1100-04.
12. Branstetter J, von Fraunhofer J.A. (1982) The physical properties and sealing action of endodontic sealer cements - A review of literature. Journal of Endodontics 8, 312-316.
13. Al Rafei S R, Sayegh F.S, Wrgiht G. (1982) Sealing ability of a new root canal filling material. Journal of Endodontics 8,152 -153.
14. Eldeniz AU, Mustafa K, Orstavik D, Dahl J E. (2003) Assessment of cytotoxity of five new root canal sealers. International Endodontics Journal 23(6), 435.
15. Callahan JR. Rosin solution of the sealing of the dentinal tubuli and as an adjuvant in the filling of root canals. Journal of the Allied Dental Societies. 1914;9:53-63.
16. Sommer RF (1946). Essential for successful root resection. Am J Orthod Oral Surg. 1946;32:76-100.
17. Marshall FJ, Massler M. (1961) The sealing ability of pulpless teeth evaluated with radioisotopes .Journal of Dental Medicine 16,172.
18. Weine FS.(1982).Endodontic Therapy, 3rd edition.
19. Goldberg F, Artaza L P, De Silvio A. (2001). Effectiveness of different obturation techniques in the filling of simulated lateral canals. Journal of Endodontics 27,362-364. |