Introduction
The conflict in the objectives of occlusion that exists in dentistry often finds its origin in semantics and in the interpretation and application of research. The most important phase of dental treatment is to restore the dentition to its best possible form and health with minimum intervention.[1]
One clinical procedure which has gained popularity in the prosthodontics sphere is the practice of “Full mouth Rehabilitation”. It implies the employment of all diagnostic, therapeutic and restorative procedures at the dentist's command for the treatment and prevention of dental diseases.[2]
Natural dentition can be categorized into two groups (D'Amico A. 1958)[3] according to their functional occlusal pattern i.e.
(i) Those individuals who exhibited occlusal contacts on several teeth on working side in eccentric mandibular excursions classified as a Group Function Occlusion (Figure 1).
(ii) Those individuals who exhibited only cuspid contacts with all the posterior teeth out of contact; on the working side in eccentric mandibular excursion has a Canine Guided Occlusion (Figure 2).
 | Figure 1 : Group function occlusion
 |
 | Figure 2 : Canine guided occlusion
|
Occlusion rehabilitation in patients with grossly attrited or severely compromised occlusion requires a proper diagnosis and treatment planning. The newer techniques developed that helps in diagnosis and treatment planning include the use of cephalometry. Different cephalometric analysis can easily guide the dentist to the prediction of the final outcome of treatment.[4]
The purpose of this study was to find the relationship of Frankfort mandibular plane angle and vertical overlap to eccentric occlusal groups.
Materials And Methods
Patient Selection Criteria
A total of 88 patients of age group 19-30 years, were screened from those attending the O.P.D of Department of Prosthodontics and amongst the student population of Sardar Patel Post Graduate Institute of Dental and Medical Sciences (SPPGIDMS) Lucknow. Of these, 34 (18 males, 16 females) were found to be falling under group function occlusion category. Out of 34, thirty patients; 15 males and 15 females matched agewise were enrolled in this group. From the remaining 54 patients, 30 patients (15 males and 15 females) matched agewise comprised the Canine guided group.
The general criteria for selecting the patients for the study was; irrespective of cast, creed, religion, with Angle's class I molar relationship, without anterior crowding, without anterior and posterior crossbite, all permanent teeth being present (excluding third molar), with good periodontal health, with optimum TMJ condition, with no history of any orthodontic treatment, and no or minimum amount of attrition.
Depending upon FMA, each group was further divided into two; one group with FMA of 15-24 degrees and second with FMA of 25-34 degrees.
Overbite
Specially designed Vernier calipers (Figure 3) was used to measure the overbite at central incisor and at canine. Mandibular teeth were dried with cotton. A lead marking pencil was used to mark the overbite at the labial surface of mandibular central incisor at level of incisal edge of central incisor (either right or left) when patient closes in CO. Distance from incisal edge of mandibular central incisor to the marked line was measured (Figure 4). Then a line was extended towards the mesiobuccal surface of mandibular canine and distance from tip of mandibular canine to the marked line was measured. Alginate impression with dentulous trays was made for each subject.
 | Figure 3 : Marking of incisal edges of maxillary incisor and canine at mandibular teeth
|
 | Figure 4 : Modified Vernier calipers at edges
|
Positioning of the Patient for Lateral Head Cephalogram
The patient was then positioned within the ear rods of the cephalostat exerting moderate pressure on the external auditory meatus. The central beam of the X-ray coincides with the transmeatal axis, i.e. with the ear rods of the cephalostat. The patient's head was placed with the Frankfort plane parallel to the floor. A nasal pointer was then secured against the bridge of the patient's nose to eliminate rotation around the ear rods in the sagittal plane.
Lateral Cephalogram analysis
Each lateral head cephalogram was analysed for FMA, IMPA, IIA, GA.[5] Case sheet for each patient was filled as a record. All data was collected for statistical analysis. The data was analyzed for mean value, standard deviation, for comparison and correlation between different groups student ‘t’ test was used, and for significance ‘P’ value was calculated.
Results
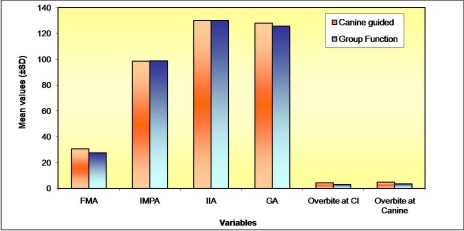
When both the groups were compared, statistically significant difference (P<0.001) was found with higher mean FMA for Canine guided occlusion group. However, no significant difference was seen in mean IMPA between the two groups, though the mean IMPA was higher in Canine guided group. The mean IIA and mean GA were found to be significantly higher in Group function occlusion. However, overbite at central incisor as well as at canine was found to be significantly higher (P<0.001) in Canine guided group as compared to Group function occlusion group (Table 1). Distribution of the sample is illustrated in (Graph 1).
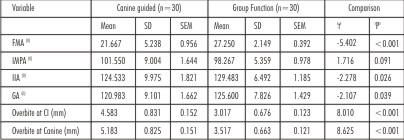 | Table 1: Comparison of cephalometric variables for Canine guided and Group function occlusion (overall) (n=60)
|
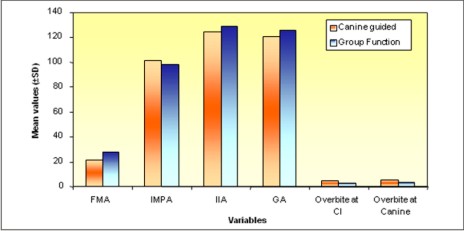 | Graph 1: Comparison of cephalometric variables for Canine guided and Group function occlusion (overall) (n=60)
|
When the sample was categorized according to FMA, 27 cases were found to be in FMA range of 15 to 24 degrees out of sixty cases. There were 24 cases in Canine guided occlusion group and 3 cases in Group function occlusion group. When two groups were compared, statistically significant (P=0.006) higher FMA was seen amongst Group function patients (Table 2, Graph 2).
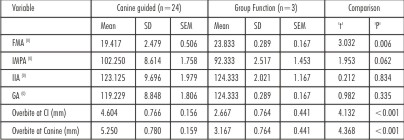 | Table 2: Comparison of cephalometric variables for Canine guided and Group function occlusion (FMA range 15 to 24) (n=27)
|
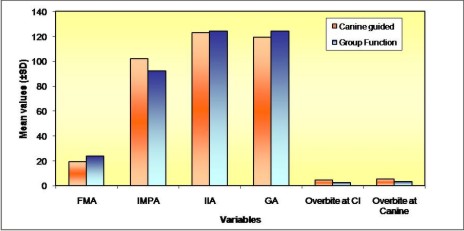 | Graph 2: Comparison of cephalometric variables for canine guided and group function occlusion (males) (n=30)
|
Out of total, 33 patients, 6 in Canine guided group and 27 in Group function group, were in FMA range 25 and above. When comparison was made between both groups, mean FMA was significantly (P=0.004) higher in Canine guided group (Table 3, Graph 3).
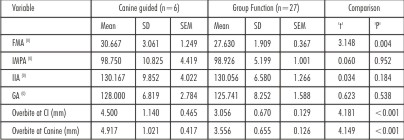 | Table 3: Comparison of cephalometric variables for Canine guided and Group function occlusion (FMA range 25 and above) (n=33)
|
 | Graph 3: Comparison of cephalometric variables for canine guided and group function occlusion (females) (n=30)
|
Discussion
A good understanding of occlusion is essential to ensure optimum dental health. But, the fact is that Occlusion is the least understood subject from past to today's modern dentistry. Occlusion is the base of dentistry, but it is often overlooked by many dentists as they may not be able to implement the concept of occlusion into the clinical practice. So, a thorough knowledge of occlusion is mandatory to achieve good, satisfactory and acceptable results in the patient.
Treating occlusal disharmonies of natural dentition is one of the most difficult jobs. Any interference between the maxillary and mandibular teeth during eccentric movements can affect the harmony of stomatognathic system. Phased treatment plans can be proposed for long term oral rehabilitation patients.
The significance of FMA in Prosthodontic diagnosis and treatment planning plays an important role in full mouth rehabilitation.[2] In this study, the comparison of cephalometric variables depending on FMA for Canine guided and Group function occlusion was made to find their relevance in occlusal rehabilitation.
Dipietro and Moergeli[6] concluded that the anterior guidance requires stable posterior contacts at the proper VDO. It requires correct lingual contours to redirect and redistribute occlusal forces during protrusive disclusion.
O' Leary[7] concluded that the mean mobility of canine in Canine protected occlusion is more than in Group function occlusion, indicating that for providing canine guided occlusion the cuspid teeth should be periodontally sound.
Cephalometrics can be of great value as a diagnostic tool when restoring the anterior dentition to proper function. The patient's anterior tooth positions can be analyzed. The plane of occlusion, skeletal classification and facial type can be determined. The exact treatment outcome depends upon the expert diagnosis and implementation of different concepts of occlusal rehabilitation. For the post treatment comfort of the patient one can use all the available diagnostic tools[2],[8], this study was a step towards the same. By using the method of cephalometry, one can implement the analysis made by the lateral cephalograms in determining the type of occlusion during the rehabilitation procedures.
Correlating with Clinical Findings of Vertical Overlap
When mean values of Canine protected and Group function occlusion were compared for central incisor and canine vertical overlap, it was observed that the canine vertical overlap had a greater mean values than incisor vertical overlap. This may be because of greater projection of cusp tips of maxillary and mandibular canines occlusally in comparasion to incisors. But, when mean values of incisor and canine vertical overlap were compared in both the groups, it was Canine protected occlusion which had greater mean values than group function occlusion. This may be argued, by the fact that the increased anterior vertical overlap is a guiding factor of the Canine protected occlusion.
When the anterior vertical overlaps were compared with the FMA, GA and IIA of the present study, they showed an inverse relation i.e. greater mean values of FMA, GA and IIA were associated with lesser mean values of overbite both at central incisor and at canine of group function occlusion group and vice versa in Canine protected occlusion. This inverse relation between vertical overlap and FMA, GA and IIA is in accordance with the study done by DiPietro.[9] This finding may be of great clinical value in deciding the amount of anterior vertical overlap (overbite) to be provided during occlusion rehabilitation.
Conclusions
1. While replacing the natural dentition, FMA can be used as a diagnostic tool in occlusal rehabilitation.
2. The comparisons made either independently (irrespective of gender) or dependent on gender; or dependent on FMA between 0-24 degrees, statistically
a) higher mean values of FMA, GA and IIA were obtained for Group function occlusion as compared to Canine guided occlusion.
b) greater overbite at central incisor and at canine was found with Canine guided occlusion as compared to Group function occlusion.
c) higher mean IMPA was for Canine guided occlusion.
3. In individuals with FMA between 25-34 degrees, statistically
a) higher mean FMA was in Group function occlusion males.
b) higher mean values of IIA, GA and overbite were found at central incisor and at canine in canine guided occlusion in females. .
c) higher mean IMPA was found in Canine guided occlusion in males.
4. An inverse relationship between FMA, GA and IIA was seen with overbite both at central incisor and at canine.
5. Along with FMA, Gonial angle can also be used as a determinant of type of eccentric occlusion.
References
1. Clark JR, Evans RD. Functional occlusion: I; A review. Br J Orthod 2001;28(1):76-81.
2. Jemt T, Lundquist S, Hedgegard B. Group function or Canine protection. J Prosthet Dent 1982;48(6):719-724.
3. D'Amico A: Functional occlusion of natural teeth of man. J Prosthet Dent 1961;11(5): 899-915.
4. Park IC, Bowman D, and Klapper L. A cephalometric study of Korean adults. Am J Orthod Dentofacial Orthop1989;96:54-59.
5. Tweed CH: Clinical Orthodontics, St Louis, 1966, The C.V. Mosby Company, Vol.1; p 2-5.
6. DiPietro GJ, Moergeli JR. Significance of Frankfort-mandibular plane angle to prosthodontics. J Prosthet Dent 1976;36(6):624-635.
7. O'Leary TJ, Shanley DB, Drake RB. Tooth mobility in cuspid-protected and group-function occlusion. J Prosthet Dent 1972;27(1):21-25.
8. Gordon J. Chirestensen: Defining Oral Rehabilitation. J.A.D.A 2004; 135, Feb: 215-217.
9. DiPietro GJ. A study of occlusion as related to Frankfort-mandibular plane angle. J Prosthet Dent 1977;38(4):452-458. |