Pain, irrespective of the cause, is most common reason for which patient seeks dental treatment. Dentist must be able to diagnose the cause and have a strategy for its management.
Successful management of pain includes
-accurate diagnose of the condition
-and appropriate dental treatment.
Appropriate dental treatment removes the condition causing pain and usually provides rapid resolution of the symptoms. In addition to the above , supportive drug therapy is given as an adjunct to relieve patient from pain. Of many dental conditions like pulpitis , gingivitis/periodontitis , pericoronitis , periapical abscess , or post extraction etc. , pain is usually caused by inflammation and infection.
In addition to antibiotics to cover the infection , anti-inflammatory (steroidal or non-steroidal) are used widely to manage the pain. Non-steroidal provides excellent relief due to their anti-inflammatory and analgesic effect.
Steroids can also be used for pain management but their use should be very selective and limited.
NSAIDs are prescribed to every patient coming for dental treatment with pain and sometimes they are prescribed even , when not required.
Since NSAIDs find place in every prescription , it is must to understand , in addition to therapeutic benefits , the safety of NSAIDs.
NSAIDs
The anti-inflammatory, analgesic and antipyretic drugs are a heterogenous group of compounds often chemically unrelated which non theless share certain therapeutic actions and side effects. They are frequently called NSAIDs. To understand the unwanted side effects , in addition to therapeutic effect as anti-inflammatory , it is important to understand the process of inflammation.
In brief, inflammation process involves a series of events that can be elicited by numerous stimuli ( e.g. infectious agents , ischemia , antigen-antibody reaction , thermal or physical injury ). Each type of stimuli provokes a characteristic pattern of response that represents a relatively minor variation.
At microscopic level , response is usually accompanied by familiar clinical signs of erythema , edema , tenderness , and pain.
Inflammatory response occurs in three phases
-acute transient phase
-delayed sub-acute phase
-chronic proliferative phase
In the body , PGs , TXs ( thromboxane) and LTs ( leukoterines ) are collectively called eicosanoids. Eicosanoids are most universally distributed autocoids in the body. Practically every cell and tissue is capable of synthesizing one or more types of PGs and LTs. There are no preformed stores of PGs and LTs. They are synthesized locally at the rate governed by the release of arachidonic acid from membrane lipids in response to appropriate stimuli.
Cyclooxygenase ( COX ) pathway generates eicosanoids ( PGs , TXs ,and Prostacyline ) , while Lipooxyganase pathways generates open chain compounds ( LTs ).
All tissues have cox , can form PGG2 , PGH2 which are unstable compounds.
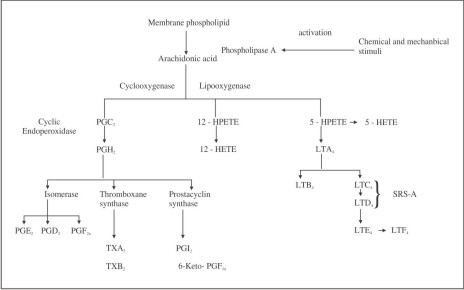 | Biosynthesis of protaglandins (PG) and leukotrienes (LT)
 |
TX- thromboxane , PGI - Prostacycline , HPETE - hydroperoxy eicosatetraenoic acid , HETE - Hydroxy eicosatetraenoic acid , SRS-A - Slow reacting substance of anaphylaxis.
Cyclooxygenase (COX)
Cox is known to exist in two forms -
Cox-1 and Cox -2 while both forms catalyse the same reactions.
A splice variant of Cox -1 ( designated as COX -3 ) has been found in dog brain. This iso-enzyme is inhibited by paracetamol but its role in human is not known.
COX - 1 is a constitutive enzyme in most cells. Its activity is not changed once the cell is fully grown.
COX - 2 on the other hand , normally present in insignificant amounts , is inducible by cytokines , growth factors , and other stimuli during inflammatory process.
It is believed that eicosanoids produced by cox-1 participate in physiological ( house keeping ) functions such as gastric mucosa , hemostasis and maintenance of renal functions while those produced by cox-2 leads to inflammation and other pathological changes.
However , certain sites in the kidney and brain constitutively express cox-2 which may play physiological role.
Cyclic eicosanoids produce a wide variety of actions depending upon the particular PGs , species on which tested , tissue , hormonal status and other factors. PGs differ in their potency to produce a given action and different PGs sometimes have opposite effects. Even the same PG may have opposite effect under different circumstances. Since , virtually all cells and tissues are capable of forming PGs , they have been implicated as mediators or modulators of a number of physiological processes and pathological status.
Side Effects Of NSAIDs
The principal basis for therapeutic action of NSAIDs is the inhibition of prostaglandin synthesis. Since different PGs , as described earlier , are implicated in different physiological functions in the body , their inhibition by the NSAIDs will have some adverse effects. So in addition to sharing many therapeutic activities , NSAIDs share several unwanted side effects as described
On Gastric Mucosa
Most common is the propensity to induce gastric or intestinal ulceration. Highly selective cox2 inhibitors lack the propensity to induce gastric or intestinal ulceration. Gastric damage is brought about by two mechanisms-
Although local irritation by oral administered drug allows back diffusion of acid into gastric mucosa and induce tissue damage , parenteral administration can also cause damage and bleeding.
In gastric mucosa , gastric prostaglandins (PGs ) especially PGI2 and PGE2 serve as cytoprotective agents. These eicosanoids inhibits acid secretion by the stomach by -
-enhancing mucosal blood flow
- promotes secretion of cytoprotective mucus in the intestine
Inhibition of synthesis of cox 1 mediated gastro protective PGs (PGE2 and PGI2) renders the stomach more susceptible to damage by inducing back diffusion of H+ ions in the gastric mucosa. Deficiency of PGs reduces mucus and HCO3- secretion , tends to enhance acid secretion and may promote mucosal ischemia. Thus NSAIDs enhance aggressive factors in the gastric mucosa and are ulcerogenic.
Side effects may range from mild dyspepsia and heart burn to ulceration sometimes with fatal results.
These side effects are produced by all NSAIDs to varying extents : relative gastric toxicity is a major consideration in the choice of NSAIDs.
On Renal Functions
Adverse effects on renal functions are well recognised with the use of non selective NSAIDs.
Role of PGs in Renal Functions
- PGE2 and PGI2 increase water , Na+ and K+ excretion and have a diuretic effects
- PGE2 have been shown to have a frusemide like inhibitory effect on Cl- reabsorption as well.
- they cause renal vasodilation and inhibit tubular reabsorption.
- PGE2 antagonises ADH action and this adds to diuretic effect .
- TXA2 cause renal vasodilation.
PGI2 , PGE2 and PGD2 evoke release of rennin.
As a result , PGs appear to function as intra-renal regulator of blood flow as well as tubular reabsorption in kidneys.
Rennin release in response to sympathetic stimulation and other influences may be facilitated by Pgs.
Effcts of NSAIDs due to inhibition of synthesis of Pgs
NSAIDs have little effects on renal function in normal condition but becomes significant in patients with CHF , hypovolemia , hepatic cirrhosis, renal disease and in patients receiving diuretics or anti- hyrertensives.
Acute renal failure may be precipitated under these circumstances because of
- COX-1 dependent impairment of renal blood flow and reduction of g.f.r. can worsen renal insufficiency.
- juxtaglomerular COX-2 dependant Na+ and water retention.
- ability to cause papillary necrosis on habitual intake.
NSAIDs promotes salt and water retention by reducing the PGs induced inhibition of both reabsorption of chloride and action of ADH. This may cause edema in some patients treated with NSAIDs. Neuropathy is uncommonly associated with long term use of individual NSAIDs.
Impairment Of Platelet Functions
COX-1 generated TXA2 - is a potent aggregating agent , and PGI2 - produced by vascular endotheliumis is an anti-aggregating prostanoids.
TXA2 produced by platelets and PGI2 produced by vascular endothelium probably constitutes a mutually antagonistic system preventing aggregation of platelets in circulation and inducing aggregation on injury , when plugging and thrombosis are needed.
NSAIDs inhibits the synthesis of both TXA2 and PGI2 , but effects on platelets TXA2 (cox-1 generated aggregating agent ) predominates.
This accounts for the ability of these drugs to increase the bleeding time.
Aspirin particularly have irreversible effect on cox activity , effect lasting for more than three days and require new platelet productions for the restoration of enzyme activity.
This side effect has been exploited in the prophylactic treatment of thromb oembolic disorders.
Acute administration of 400-800mg of selective cox-2 inhibitor (celecoxib) in human beings has been found to suppress PGI2 production by about 80% , without inhibiting cox-1 generated TXA2 production and platelet aggregation.
This suggests that cox-2 is a major source of PGI2 production in vivo. Since an important action of PGI2 is thought to be suppression of platelet activation , alteration of TXA2/PGI2 ratio that accompanies selective inhibition of cox2 is theoretically prothrombotic. Clinical relevance of this finding remains to be determined but can be considered when choosing an NSAIDs for the treatment of patients particularly prone to thrombotic events.
On Broncheal Muscles
In general , PGFs and PGD2 contracts and PGE2 relax bronchial and tracheal muscles.
PGE2 and PGI2 produce broncho-dilation.
TXA2 constricts human bronchial smooth muscles.
LTC4 and LTD4 are broncho constrictor in many species including humans.
Asthma may be induced due to imbalance between dilators PGs and constrictors Lts. In few individuals , aspirin like drugs including cox 1 inhibitors , consistently induce asthma possibly by diverting arachidonic acid to produce excess LTs. This sensitivity is not shared by selective cox-2 inhibitors indicating that suppression of cox-1 at the pulmonary site is responsible for the reaction.
Other Side Effects
- Intolerance
Certain individuals display intolerance to aspirin and most NSAIDs. This is manifest by symptoms that range from vasomotor rhinitis with profuse watery secretion , angioneurotic edema , generalized urticaria , and bronchial asthma to laryngeal edema and broncho constriction , flushing , hypotension , and shock. These reactions are not limited to aspirin. An individual who exhibits intolerance to aspirin will also react when given any of other NSAIDs , despite their chemical diversity , thereby ruling out immunological basis for this reaction. Inhibition of COX with consequent diversion of arachidonic acid to LTs may be involved , but there is no proof.
-Prolongation of gestation by NSAIDs
Synthesis of prostaglandins increases dramatically in the hours before parturition. PGs are thus postulated to have a major role in the initiation and progression of labour and delivery. So , inhibition of synthesis of PGs can delay and retard labour. However, labour can occur in the absence of Pgs.
Accordingly some NSAIDs have been used as tacolytic agents to inhibit pre term labour.
-NSAIDs in pregnancy and lactation
The use of analgesics during pregnancy has been recently reviewed , and the findings are summarized in the Table 1.
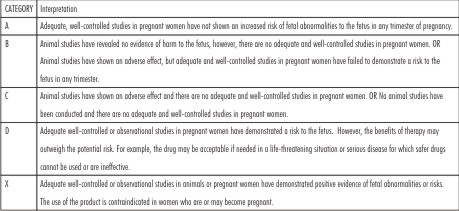 | FDA CATEGORY FOR DRUG USE IN PREGENCY
|
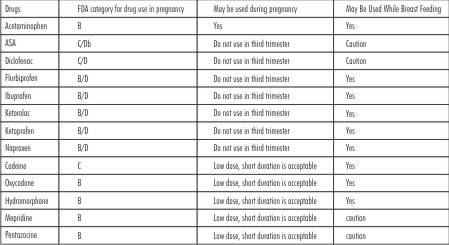 | ANALGESIC USE IN PREGNANCY OR LACTATION
|
Optimal management of dental pain during pregnancy is removal of the source of pain using local anesthesia. If , however , post operative pain is present , an analgesic may be necessary and should be made available. Acetaminophen is clearly the analgesic of choice in all stages of pregnancy. The use of NSAIDs , including ASA , is less favourable , particularly late in pregnancy. NSAIDs may predispose to ineffective contractions during labour , increased bleeding during delivery or premature closure of ductus arteriosus of the heart. NSAIDs are therefore contraindicated in the third trimester .
If acetaminophen is insufficient , opioids are considered acceptable during pregnancy provided they are given for a short duration . Chronic opioid use can result in fetal dependence, premature delivery & growth retardation. As with pregnancy, acetaminophen is the analgesic of choice in lactation. ASA and diclofenac may increase bleeding and should be avoided if possible. Opioids are considered safe in lactation.
 |
|
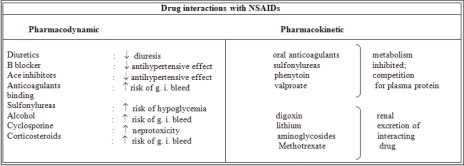
Choice Of NSAIDs
Vast majority of NSAIDs are organic acids and act as reversible competitive inhibitors of cyclooxygenase activity. However , these drugs do not inhibit the metabolism of arachidonate by lipooxygenase. In fact , inhibition of COX theoretically could lead to increased formation of leukotrienes by increasing the amount of arachidonate that is available to lipooxygenase.
Cox 1 and Cox 2 differ in their sensitivity to inhibition by certain anti-inflammatory drugs. This observation has led to the recent development of clinically useful agents that selectively inhibit Cox-2. These drugs show distinct therapeutic advantages over non selective NSAIDs agents , since COX- 2 is predominant cyclooxygenase at the site of inflammation but not at sites such as gastrointestinal tract. Thus, cox2 inhibitors are anti-inflammatory but do not possess many of the adverse side effects of non selective cyclooxygenase inhibitors.
NSAIDs have their spectrum of adverse effects. They differ quantitatively among themselves in producing different side effects and there are large inter- individual variation. No single drug is superior to others for every patient. Choice of the drug is inescapably empirical.
The cause and nature of pain (mild , moderate or severe ; acute or chronic ; ratio of pain ; inflammation) along with consideration of risk factors in the given patient govern the selection of analgesic. Also to be considered are past experience of the patient, acceptability and individual preference. Patients differ in their analgesic response to different NSAIDs. If one NSAIDs is unsatisfactory in a patient , it does not mean that other will also be unsatisfactory. Some subjects feel better on a particular drug , but not on a closely related ones. It is in this context that availability of such a wide range of NSAIDs may be welcomed.
References
1. GOODMAN & GILLMAN'S - The pharmacological basis of Therapeutics-Tenth Edition
2. ROBBINS - Pathological basis of Diseases -Sixth Edition
3. K.D TRIPATHI - Essentials of Medical Pharmacology - Sixth edition
4. UPDENT April - June 2009 ; Vol : 8 , Number 1 |