Introduction
Dens invaginatus is a developmental anomaly resulting from the invaginations of the enamel organ into the dental papilla during the soft tissue stage of development. As the hard tissues are formed, the invaginated enamel organ produces a small tooth within the future pulp chamber. This kind of tooth malformation was described first by Ploquet in 1794 who discovered this anomaly in a whale's tooth1.
Dens invagination in a human tooth was first described by a dentist named 'Socrates' in 1856 2. Synonyms for this malformation are: Dens in dente, invaginated odontome, dilated gestant odontome, dilated gestant odontome, dilated composite odontome, tooth inclusion, dentoid in dente, gestant odontome, dents telescopes.
Aetiology
The aetiology of dens invaginatus malformation is controversial and remains unclear. Over the last decades several theories have been proposed to explain the aetiology of dental coronal invaginations:
Kronfeld (1934) suggested that the invagination results from a focal failure of growth of the internal enamel epithelium while the surrounding normal epithelium continues to proliferateand engulf the static area3.
Rushton (1937) proposed that the invagination is a result of rapid and aggressive proliferation of a part of the internal enamel epithelium invading the dental papilla. He regarded this as benign neoplasma of limited growth4.
Oehlers (1957) considered that distortion of the enamel organ during tooth development and subsequent protrusion of a part of the enamel organ will lead to the formation of an enamel-lined channel ending at the cingulum or occasionally at the incisal tip. The latter might be associated with irregular crown form5,6.
Atkinson (1943) suggested that the problem was the result of external forces exerting an effect on the tooth germ during development7. Such forces could be from adjacent tooth germs, e.g. the central incisor or canine which develop at least 6 months prior to the lateral incisor8 whilst other external factors such as trauma9 and infection10 have also been suggested as a cause.
During tooth development the ectomesenchymal signalling systems that occur between the dental papilla and the internal enamel epithelium affect tooth morphogenesis11. These signals have specific roles such as the regulation of growth and the folding of the enamel organ12. The absence of certain molecules can result in abnormally shaped teeth as well as defects in the developing tooth germ13. For this reason the proposal that genetic factors may be the cause of dens invaginatus has some credibility14-16. Support for this possible cause also comes from a reported case of an individual lacking chromosome 7q32 who presented with dens invaginatus in addition to other dental abnormalities such as hypodontia17. There is further support from a clinical study of 3020 Swedish children that reported 2.7% of patients with dens invaginatus, 43% of their parents and 32% of siblings also had evidence of the condition14.
Classification
The first documented attempt to classify dens invaginatus was by Hallet18 (1953) who suggested the existence of four types of invagination based on both clinical and radiographic criteria. Other classifications have also been described involving a variety of criteria and standards19,20. For example, Schulze & Brand21 (1972) suggested an assessment based on twelve possible variations in clinical and radiographic appearance of the invagination. However, the system described by Oehlers5 (1957a) appears to be the most widely used, possibly because of its simple nomenclature and ease of application. This system categorizes invaginations into three classes as determined by how far they extend radiographically from the crown into the root (Figure 1).
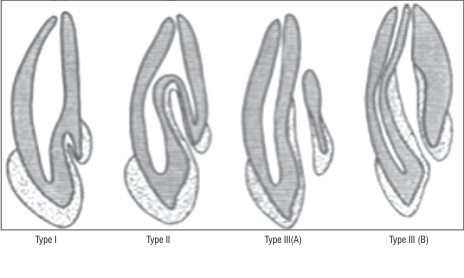 | Figure 1: Oehler's classification of dens invaginatus (Coronal types)
 |
Type I: The invagination is minimal and enamel-lined, it is confined within the crown of the tooth and does not extend beyond the level of the external amelo-cemental junction.
Type II: The invagination is enamel-lined and extends into the pulp chamber but remains within the root canal with no communication with the periodontal ligament .
Type IIIA: The invagination extends through the root and communicates laterally with the periodontal ligament space through a pseudo-foramen. There is usually no communication with the pulp, which lies compressed within the root.
Type IIIB: The invagination extends through the root and communicates with the periodontal ligament at the apical foramen. There is usually no communication with the pulp.
In Type III lesions, any infection within the invagination can lead to an inflammatory response within the periodontal tissues giving rise to a ‘peri-invagination periodontitis’.
The limitations associated with the use of conventional radiography in the classification and management of dens invaginatus may be overcome in the future with the increasing availability of computerized 3D imaging22,23. Currently, such clinical techniques do not provide images of sufficient quality to fully evaluate the morphology of an invagination in situ although for extracted teeth sufficient detail can be obtained.
Prevalence and Distribution
The reported prevalence of adult teeth affected with dens invaginatus is between 0.3% and 10% with the problem observed in 0.25% to 26.1% of individuals examined (Table 1). The wide variation in reported prevalence may be explained by the different cohorts studied, identification criteria used and diagnostic difficulties However, more recent studies24,25 have utilized a recognized classification system.
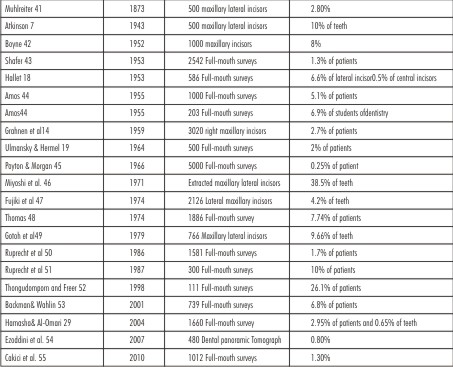 | Table 1: Prevalence Studies On Dens Invaginatus
|
The permanent maxillary lateral incisor appears to be the most frequently affected tooth26 with posterior teeth less likely to be affected27,28. This is supported by Hamasha & Al-Omari29 (2004). A number of case reports have identified dens invaginatus in mandibular teeth30-34.There is also some evidence that the problem may be symmetrical7,14,24. However, conflicting opinions exist with Swanson & McCarthy35 (1947) . There have also been case reports of dens invaginatus occurring in the primary dentition36-39.
However, all the documented case reports are of males which, if a true reflection, contrasts to the permanent dentition where females appear to be more at risk40 or there is no gender difference reported24. The dental literature on dens invaginatus malformations contains several case reports presenting invaginated teeth coincident with other dental anomalies, malformations and even dental or medical syndromes.26 (Table 1).
Nature of Invagination
The invagination may be associated with changes in the morphology of the root canal itself. One study that examined an extracted root filled invaginated tooth observed that the root canal was irregular in cross-section, with wave-like constrictions and dilatations56. There have also been reports of multiple root canals being present in association with the invagination57-59. Investigations into the histological, microscopically and radiographical nature of dens invaginatus have provided conflicting results. In some studies, the invaginated surface has been described as being uniform and regular with no communication with the pulp60-63. In contrast, others have described interruptions in the invaginated surface which could potentially act as a portal for irritants to the pulp 3,5,9,61,63,64. Beynon 65 reported hypomineralized enamel at the base of the invagination where as Morfis 66 in a chemical analysis, detected up to eight times more phosphate and calcium compared with the outer enamel, but in his analysis magnesium was missing completely. Bloch -Zupan et al67 found differences in structure and composition between the external and internal enamel. The internal enamel exhibited a typical and more complex rod shapes and its surface presented the typical honey comb pattern but no perikymata which however was observed on the outer surface of tooth.The structure of the dentine surrounding the invagination has also been reported as being irregular with connective tissue inclusions and communications towards the pulp7,60,62,65.
The variation in findings of the nature of the invagination can possibly be explained by the different techniques used in each study, namely, histological62 chemical analyses66, SEM67,68 and microradiographic65 and micro X-ray diffraction60 techniques employed.
Diagnosis of Dens Invaginatus
In most cases a dens invaginatus is detected by chance on the radiograph (Figure 2). Clinically, unusual crown morphology ('dilated', 'peg-shaped', 'barrel-shaped') or a deep foramen coecum may be important hints, but affected teeth also may show no clinical signs of the malformation. As pulpal involvement of teeth with coronal invaginations may occur a short time after tooth eruption early diagnosis is mandatory to instigate preventive treatment.
 | Figure 2: Radiographic appearance of different types of dens invaginatus (a) Type I DI, Note the deep fissuring pointing towards the pulp. (b) Type II DI, Note the tearshaped ribbon-like formation of the invagination cavity. (c) Type III (A) DI
|
The invagination allows entry of irritants into an area which is separated from pulpal tissue by only a thin layer of enamel and dentine and presents a predisposition for the development of dental caries. In some cases the enamel-lining is incomplete. Channels may also exist between the invagination and the pulp3,69. Therefore, pulp necrosis often occurs rather early, within a few years of eruption, sometimes even before root end closure19,35,70. Other reported sequelae of undiagnosed and untreated coronal invaginations are abscess formation 71-73, retention of neighbouring teeth 74,75, cysts 27,71 and internal resorption 76
Normal conventional radiograph can not provide detailed structural information about this malformation.
A latest radiographic technology, spiral computed tomography, have been introduced by Reddy et al which is not only helpful in diagnosis of dens invaginatus but also provide3-dimensional image of variations in root canal anatomy. 77
Management of dens invaginatus
The treatments options are;
1) Prophylactic or preventive sealing of the invagination 78,79
2) Root canal treatment 34,80
3) Endodontic apical surgery 81,82
4) Intentional replantation 83
5) Extraction 43,84
Type I and Type II
Once an invagination has been identified, base-line vitality test readings should be taken to get current pulpal status. Where pathological disease is absent the instigation of appropriate prophylactic measures should commence as soon as possible. There have been a wide variety of techniques advocated for prophylactic treatment. This has included the preparation of the invagination entrance and the placement of an amalgam restoration whilst more contemporary techniques have included the use of fissure sealant. 85,86 Where possible the use of magnification to open up the invagination entrance using a combination of fast hand piece burs and ultrasonic instruments should be considered to gain full access to the invagination.84 Once the invagination is fully exposed, MTA can be used to obturate the invagination and access cavity will be sealed with composite The tooth should be regularly monitored for vitality loss. If this arises, appropriate root canal treatment should be instigated.85
Antiseptic control is usually achieved by intracanal medicaments such as calcium hydroxide most commonly used but recently introduced triple antibiotic (ciprofloxacin,metronidazole,minocycline) paste has also been used and open apex problem is overcome by forming apical plug either using calcium hydroxide or by MTA (mineral trioxide aggregate).34,87,88 When simple endodontic therapy fails then combination of nonsurgical and surgical treatment could be performed.81
Type III
In a vital tooth associated with periradicular inflammation, the invagination should be treated endodontically in the same way as anormal root canal to preserve the pulp vitality.89 A combined endodontic and surgical therapy in a vital tooth has also been reported.82 Pulp necrosis occurring in a tooth with the usual form of type III invagination is often successfully managed by endodontic therapy of root canal and the invagination alone, or by a combined endodontic and surgical therapy.90,91 In some cases ultrasonic can be used for the complete removal of invagination to facilitate endodontic therapy.84
As the morphology of these teeth is complex, if root canal treatment is not possible then extraction is usually recommended and prosthetic replacement is done.85,92 The role of intentional replantation has also been reported in very complex forms of type III dens invaginatus.93,94 The use of MTA in combination with gutta percha may be considered, where the post preparation apical portions are wide and blunder-buss in their formation.95
References
1. Westphal A. Ein kleines Kuriosum um den ersten 'Dens in dente'. Zahnärztliche Mitteilungen 1965; 55, 1066-70.
2. Shulze C.Developmental abnormalities of the teeth and the jaws In:Gorlin O, Goldman H .Thoma's Oral Pathology.1970.St.Louis:Mosby. p. 96-183.
3. Kronfeld R. Dens in dente. J Dent Res 1934;14:49-66.
4. Rushton MA. A collection of dilated composite odontomas. Brit Dent J 1937;63:65-85.
5. Oehlers FA. Dens invaginatus. I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol 1957;10:1204-18.
6. Oehlers FA . Dens invaginatus. II. Associated posterior crown forms and pathogenesis. Oral Surg Oral Med Oral Pathol 1957;10:1302-16.
7. Atkinson SR. The permanent maxillary lateral incisor. Am J Orthod 1943;29:685-98.
8. Segura JJ, Hattab F, R?´os V Maxillary canine transpositions in two brothers and one sister: associated dental anomalies and genetic basis. J Dent Child 2002;69:54-8.
9. Gustafson G, Sundberg S Dens in Dente. Brit Dent J 1950;88:83-8, 111-122, 144-6.
10. Sprawson EC. Odontomes. Brit Dent J1937;62:177-201.
11. Ohazama A, Courtney JM, Sharpe PT, Rank and Rankl in tooth development: co-ordination of odontogenesis and osteogenesis. J Dent Res 2004;83:241-4.
12. Kettunen P, Laurikkala J, Ita¨ranta P, Vainio S, Itoh N, Thesleff I Associations of FGF-3 and FGF-10 with signaling networks regulating tooth morphogenesis. Dev Dyn 2000;219:322-32.
13. Dassule HR, Lewis P, Bei M, Maas R, McMahon AP. Sonic hedgehog regulates growth and morphogenesis of the tooth. Development 2000;127: 4775-85.
14. Grahnen H, Lindahl B, Omnell K. Dens invaginatus. I. A clinical roentgenological and genetical study of permanent upperlateral incisors. Odontol Revy 1959;10:115-37.
15. Casamassimo PS, Nowak AJ, Ettinger RL, Schlenker DJ. An unusual triad: microdontia, taurodontia, and dens invaginatus. Oral Surg Oral Med and Oral Pathol 1978;45:107-12.
16. Hosey MT, Bedi R. Multiple dens invaginatus in two brothers. Endod Dent Traumatol 1996;12: 44-7.
17. Pokala P, Acs G. A constellation of dental anomalies in a chromosomal deletion syndrome (7q32): case report. Pediatr Dent 1994;16:306-9.
18. Hallet GE. The incidence, nature and clinical significance of palatal invagination in the maxillary incisors teeth. Proc R Soc Med 1953;46: 491-9.
19. Ulmansky M, Hermel J. Double dens in dente in a single tooth. Oral Surg Oral Med and Oral Pathol 1964;17: 92-7.
20. Vincent-Townend J. Dens invaginatus. J Dent1974;2: 234-8.
21. Schulze C, Brand E. Uber den Dens Invaginatus (Dens in dente). Zahna¨ rztliche Welt, zahna¨ rztliche Reform, ZWR 1972;81, 569-73, 613-20, 653-60, 699-703.
22. Vannier MW, Hildebolt CF, Conover G, Knapp RH, Yokoyama-Crothers N, Wang G. Threedimensional dental imaging by spiral CT. A progress report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;84: 561-70.
23. Sponchiado EC Jr, Ismail HA, Braga MR, de Carvalho FK, Simo˜es CA. Maxillary central incisor with two root canals: a case report. J Endod 2006;32:1002-4.
24. Ridell K, Meja`re I, Matsson L. Dens invaginatus: a retrospective study of prophylactic invagination treatment. Int J Paediatr Dent 2001;11: 92-7.
25. Backman B, Wahlin YB. Variations in number and morphology of permanent teeth in 7-year-old Swedish children. Int J Paediatr Dent 2001;11:11-7.
26. Hu¨ lsmann M . Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J1997;30:79-90.
27. Conklin WW. Bilateral dens invaginatus in the mandibular incisor region. Oral Surg Oral Med Oral Pathol 1978;45: 905-8.
28. Lee AM, Bedi R, O'Donnell D. Bilateral double dens invaginatus of maxillary incisors in a young Chinese girl Aust Dent J 1988;33: 310-2.
29. Hamasha AA, Al-Omari QD. Prevalence of dens invaginatus in Jordanian adults. Int Endod J 2004;37:307-10.
30. Altinbulak H, Ergu¨. Multiple dens invaginatus. Oral Surg Oral Med Oral Pathol 1993;76: 620-2.
31. Bramante CM, de Sousa SM, Tavano SM. Dens invaginatus in mandibular first premolar. Oral Surg Oral Med Oral Pathol 1993;76:389.
32. Khabbaz MG, Konstantaki MN, Sykaras SN. Dens invaginatus in a mandibular lateral incisor. Int Endod J 1995;28:303-5.
33. Hartup GR. Dens invaginatus type III in a mandibular premolar. Gen Dent1997;45:584-7.
34. Er K, Kus¸ tarci A, Ozan U, Tas¸ demir T.Nonsurgical endodontic treatment of dens invaginatus in a mandibular premolar with a large periradicular lesion: a case report. J Endod 2007;33:322-4.
35. Swanson WF, McCarthy FM.) Bilateral dens in dente. J Dent Res1947;26:167-71.
36. Rabinowitch BZ. Dens in dente: primary tooth-report of a case. Oral Surg Oral Med Oral Pathol 1952;5:1312-4.
37. Holan G. Dens invaginatus in a primary canine: a case report. Int J Paediatr Dent1998;8: 61-4.
38. Kupietzky A. Detection of dens invaginatus in a one-year old infant. Pediatr Dent 2000;22:148-50.
39. Eden EK, Koca H, Sen BH. Dens invaginatus in a primary molar: report of case. ASDC J DentChild 2002;69:49-53.
40. Thongudomporn U, Freer TJ. Prevalence of dental anomalies in orthodontic patients. Austr Dent J1998;43:395-8.
41. MuhlreiterE.Die Natur der anomalen Hohlenbildung imoberen Seitenschneidezahne. Deutsche Vierteljahresschrift für Zahnilkunde. 1873; 13:367-72.
42. Boyne PJ.Dens in dente: report of three cases.J Am Dent Assoc 1952; 45:209-10.
43. Shafer WG. Dens in dente. NY State Dent J 1953; 19: 220-5.
44. Amos ER. Incidence of the small dens in dente. J Am Dent Assoc1955; 51: 31-3.
45. PoytonGH,MorganGA.Densin dente.Dent Radiogr Photogr 1966;39:27-33.
46. Miyoshi S, Fujiwara J, Nakata T, Yamamoto K, Deguchi K. Dens invaginatus in Japanese incisors. Shika Kiso Igakkai Zasshi 1971;13:539-44.
47. Fujiki Y, Tamaki N, Kawahara K, Nabae M.Clinical and radiographicobservations of dens invaginatus. Dentomaxillofac Radiol1974;3:343-8.
48. Thomas JG. A study of dens in dente. Oral Surg Oral Med Oral Pathol 1974; 38:653-5.
49. Gotoh T, Kawahara K, Imai K, Kishi K, Fujiki Y.Clinical and radiographic study of dens invaginatus. Oral Surg Oral Med Oral Pathol 1979; 48: 88-9.
50. Ruprecht A, Batniji S, Sastry K, El-Neweihi E .The incidence of dental invagination. J Pedod 1986;10: 265-272.
51. Ruprecht A, Sastry K, Batniji S, Lambourne A. The clinical significance of dental invagination. J Pedod 1987;11:176- 81.
52. Thongudomporn U, Freer TJ. Prevalence of dental anomalies in orthodontic patients. Aust Dent J 1998; 43:395-8.
53. Backman B, Wahlin YB.Variations in number and morphology of permanent teeth in 7-year-old Swedish children. Int J Paediat Dent 2001; 11:11-7.
54. Ezoddini AF, Sheikhha MH, Ahmadi H. Prevalence of dental developmental anomalies: a radiographic study. Community Dent Health 2007; 24:140-4.
55. Cakici F,Celiekoglu M,Arslan H,Topcuoglu HS,Erdogan AS.Assessment of the prevalence and characteristics of dens invaginatus in a sample of Turkish Anatolian population. Med Oral Patol Oral Cir Bucal 2010;15:855-8.
56. De Smit A, Demaut L. Nonsurgical endodontic treatment of invaginated teeth. J Endod 1982;8: 506-11.
57. Walvekar SV, Behbehani JM. Three root canals and dens formation in a maxillary lateral incisor: a case report. J Endod1997;23:185-6.
58. de Sousa SM, Bramante CM. Dens invaginatus: treatment choices. Endod Dent Traumatol 998;14:152
59. Pai SF, Yang SF, Lin LM. Nonsurgical endodontic treatment of dens invaginatus with large periradicular lesion: a case report. J Endod 2004;30:597-600.
60. Brabant H, Klees L. Beitrag zur Kenntnis der 'dens in dente' benannten zahnanomalie. Stoma 1956;9:12-27.
61. Omnell KA, Swanbeck G, Lindahl B. Dens invaginatus. II. A microradiographical, histological and micro X-ray diffraction study. Acta Odontol Scand 1960;18:303-30.
62. De Smit A, Jansen HW, Dermaut L. An histological investigation of invaginated human incisors. J Biol Buccale 1984;12:201-9.
63. Piatelli A, Trisi P. Dens invaginatus: a histological study of undemineralized material. Endod Dent Traumatol 1993;9:191-5.
64. Hitchin AD, Mchugh WD. Three coronal invaginations in a dilated composite odontome. Brit Dent J 1954;97: 90-2.
65. Rushton MA. Invaginated teeth (dens in dente): Contents of the invagination. Oral Surg Oral Med Oral Pathol 1958;11:1378-87.
66. Beynon AD. Developing dens invaginatus (dens in dente). A quantitative microradiographic study and a reconsideration of the histogenesis of this condition. Brit Dent J 1982;153: 255-60.
67. Morfis AS. Chemical analysis of a dens invaginatus by SEM microanalys J Clin Pediatr Dent 1993;17:79-82.
68. Bloch-Zupan A, Cousandier L, Hemmerle J, Obry-Musset AM, Maniere MC. Electron microscopical assessments (FDI abstract FC-11# 123). Int Dent J 1995;45:306.
69. Stamfelj I, Kansky AA, Gaspersic D. Unusual variant of type 3 dens invaginatus in a maxillary canine: a rare case report. J Endod 2007;33: 64-8.
70. Hitchin AD, MCHugh WD. Three coronal invaginations in a dilated composite odontome. Brit Dent J 1954;97:90-2.
71. Nik-Hussein NN. Dens invaginatus: Complications and treatment of non-vital infected tooth. J Clin Pediatr Dent 1994;18:303-6.
72. Greenfeld RS, Cambruzzi JV. Complexities of endodontic treatment of maxillary lateral incisors with anomalous root formation. Oral Surg Oral Med Oral Pathol 1986;62:82-8.
73. ChenRJ, Yang JF, Chao TC. Invaginated tooth associated with periodontal abscess. Oral Surg Oral Med Oral Pathol 1990;69: 659.
74. Whyman RA, Macfadyen EE. Dens in dente associated with infective endocarditis. Oral Surg Oral Med Oral Pathol 1994;78:47-50.
75. Conklin WW. Double bilateral dens invaginatus in the maxillary incisor region. Oral Surg Oral Med Oral Pathol 1975;39:949-52.
76. Mader C. Triple dens in dente. Oral Surg Oral Med Oral Pathol 1977;44:966.
77. Reddy YP, Karpagavinayagam K, Subbarao CV.Management of Dens invaginatus diagnosed by spiral computed tomography. J Endod 2008; 34:1138-1142.
78. ShapiroL. Dens in dente. Oral Surg Oral Med Oral Pathol 1970; 30:782.
79. Aguiar CM, Ferreira JP, Câmara AC, de Figueiredo JA. Type 2 dens invaginatus in a maxillary lateral incisor: a case report of a conventional endodontic treatment. J Clin Pediatric Dent. 2008; 33:103-6.
80. Steffen H, Splieth C. Conventional treatment of dens invaginatus in maxillary lateral incisor with sinus tract: one year follow-up. J Endod 2005; 31:130-3.
81. Ortiz P, Weisleder R, Villareal de Justus Y. Combined therapy in the treatment of dens invaginatus: case report. J Endod 2004; 30:672-4.
82. Nallapati S.Clinical management of a maxillary Lateral incisor with vital pulp and type III dens iinvaginatus;a case report.J Endod 2004;30:726-31.
83. Nedley MP, Power GK. Intentional extraction and reimplantationof an immature invaginated central incisor. ASDC J Dent child 1997;64:417-20.
84. Girsch WJ, Mc Clammy TV. Microscopic removal of dens invaginatus. J Endod 2002; 28:336-9.
85. Alani A .Dens invaginatus;a problem from the outside in.Int Dent J 2009;59(6):343-8.
86. Bishop k,Alani A.Densinvaginatus.part 2:Clinical,radiographic features and management options. Int Endod J 2008;41: 1137-54.
87. Schmitz MS, Montagner F, Flores CB,Morari VHC et al. Management of dens invaginatus type I and open apex. Report of three cases.J Endod 2010;36:1079-1085.
88. Kristofferson O, Nag OH, Fristad. Dens invaginatus and treatment options based on a classification system: report of a type II invagination. Int Endod J 2008;41:702-9.
89. Tsurumachi T.Endodontic treatment of an invaginated maxillary lateral incisor with a periradicular lesion and a healthy pulp. Int Endod J 2004;37:717-23.
90. Jung M.Endodontic treatment of dens invaginatus type III with three root canals and open apical foramen.Int Endod J 2004;37:205-13.
91. Carounandy U,Sathyanarayanan R.Dens invaginatus:two cases.Endodontology 2000;12:86-9.
92. Demartis P, Disso C, Cotti M, Cotti E. Endodontic treatment and hypotheses on an unusual case of dens invaginatus. J Endod. 2009; 35(3):417-21.
93. Bansal M, Singh NN, Singh AP. A rare presentation of dens in dente in the mandibular third molar with extra oral sinus. J Oral Maxillofac Pathol 2010;14:80-2.
94. Arsenault M,Andreasen RD et al.Facial cellulitis secondary to dens invaginatus :a case report. J Can Dent Assoc 2010;76:a114.
95. Silberman A, Cohenca N, Simon JH. Anatomical redesign for the treatment of dens invaginatus type III with open apexes: a literature review and case presentation. J Am Dent Assoc 2006; 137(2):180-5. |