INTRODUCTION
A temporary anchorage device (TAD) is a device that is temporarily fixed to bone for the purpose of enhancing orthodontic anchorage either by supporting the teeth of the reactive unit or by obviating the need for the reactive unit altogether, and which is subsequently removed after use.
They can be located transosteally, subperiosteally or endosteally; and they can be fixed to bone either mechanically (cortically stabilized) or biochemecially (osseointegrated). It should also be pointed out that dental implants placed for the ultimate purpose of supporting prosthesis, regardless of the fact that they may be used for orthodontic anchorage, are not considered temporary anchorage devices since they are not removed and discarded after orthodontic treatment. By using dental implants and temporary anchorage devices for orthodontic purposes we are able to obtain zero anchorage loss1.
The selection of a proper anchorage is an essential factor for the successful orthodontic treatment. Every orthodontic device, which exercises a force onto the tooth, generates an opposite force which then affects the anchorage. The implant in the bone remains stable, which ensures a secure anchorage when no teeth are used.
HISTORICAL BACKGROUND
Gainsforth and Higley suggested using metallic screws as anchors as long as 19452. Following the successful use of conventional prosthodontic implants, osseointegrated implants were used for intraoral orthodontic anchorage. Creekmore and Eklund in 1983 were the first to introduce screws in clinical orthodontics for the sole purpose of orthodontic anchorage3. In the 1990s, surgical screws (also referred to as mini-screws, mini-implants and micro-screws) increasingly were used to provide anchorage for orthodontic tooth movement. Both animal and human studies provided a basis for their clinical use. Mini-screw implants, often referred to as temporary anchorage devices (TADs), have become an accepted component of orthodontic treatment. The comparatively simple technique for the placement of these mini-screws is described with emphasis on the importance of correct site selection as well as an understanding of the possible complications that may arise.
Use of TADs in orthodontics
Temporary anchorage devices (TADs) for orthodontic anchorage are widely accepted. They are changing the way orthodontists treat some patients’ malocclusions. TADs provide a fixed point from which to apply force to move teeth. They can be placed in many different sites in the mouth. Placement is customized for each patient. TADs may contribute to predictable results, shorter treatment time and completion of active treatment on schedule.
 | Figure 1 TAD range from 6-12 mm in Length
 |
There is little or no discomfort when a TAD is placed. Caring for your TAD generally requires only routine brushing..Although small, the TAD does a big job of helping the orthodontist to move teeth predictably into their optimal positions without anchorage loss TADs are titanium-alloy mini-screws, ranging from 6 to 12 millimeters in length and 1.2 to 2millimeters in diameter. They are fixed to bone temporarily to enhance orthodontic anchorage. Titanium alloys have been used as joint replacements and for dental implants for many years. These alloys are not rejected by the body. Orthodontists often use holding arches, also known as space maintainers, and headgear to control anchorage and minimize the movement of certain teeth while carrying out the desired movement of other teeth. TADs allow orthodontists to overcome limitations of holding arches and headgears and to perform difficult tooth movements predictably. TADs can also provide a point of anchorage for patients with missing teeth.
 | Figure 2-Placement of a TAD or a mini implant in the bone
|
Site for implant placement
TADs are placed in the bone between the roots of the teeth and can be placed in the bone in the roof of the mouth as well.
Procedure for implant placement
Placement is minimally invasive and often completed using only topical anesthetic. TADs are inserted directly into the bone using a special instrument. There is little or no discomfort because there are no nerve endings in the bone tissue. Once placed, the orthodontist is able to use the TAD as orthodontic anchorage immediately. Because of the possibility that TADs can loosen or fall out, patients should avoid picking or pulling at the TAD. If the TAD does become loose or come out, call your orthodontist as soon as possible
 | Figure 3-The site for the TAD is selected
|
 | Figure 4-The TAD immediately after placement.
|
Because orthodontists have the training and expertise to place them, many orthodontists place TADs themselves. This ensures the TAD is placed exactly where the orthodontist wants it. Some orthodontists may choose to have a TAD placed by another dental specialist.
 | Figure 5-A TAD/ Implant as an anchor
|
Duration for the TAD.
The orthodontist decides about how long a TAD will be needed. It may be required only for a few months, or it may be needed throughout your orthodontic treatment. TADs are versatile and may be used in different areas of the mouth during different parts of treatment
Age considerations
TADs are placed on patients who have permanent teeth. Patients with active periodontal (gum) disease may not be candidates for TADs4.
Clinical usage of TADs for various orthodontic applications.
A typical First premolar extraction case
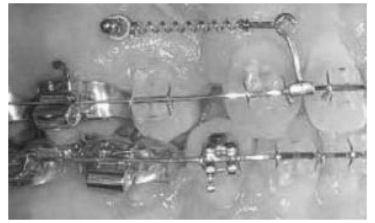 | Fig 6- Implant used for Retraction
|
A mini implant deployed between roots of the 2nd premolar and first molar for absolute anchorage during en mass retraction5,6
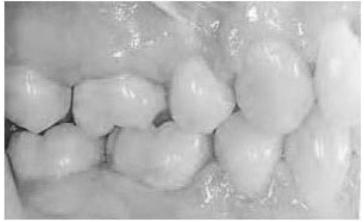 | Figure 7-Retraction completed with no anchor loss
|
Other Orthodontic Applications of TAD’S
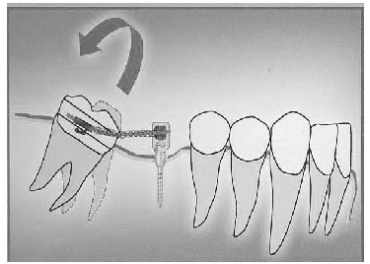 | Figure 8-Use of a micro implant for molar uprighting
|
 | Figure 9-Use of micro implants for incisor intrusion
|
 | Figure 10- Implants used for Retraction used for canine and en-mass retraction
|
 | Figure 11- Implants for Intrusion of a segment
|
SUCCESS AND FALIURE OF TAD'S
Success in microimplant orthodontics is defined as a microscrew with minimal mobility and inflammation and the ability to obtain full functional correction either through direct or indirect anchorage. In 1999, Park and Kim7 reported a success rate of 82% after 5 months of observation. In 2003 a 93% success rate was reported during a 15.8 month observation period8. Other studies have shown a similar level of success9-11. Microimplant orthodontics has a learning curve; with more experience, the success rate increases.
Regarding the causes of microimplant failure, Miyawaki et al9. reported that small diameter of the screw (<1.0mm), inflammation, and a high MPA are risk factors for the screw s placed in the mandibbular posterior teeth area Cheng et al10 found that the mandibular posterior teeth area and nonkeratinized mucosa are also risk factors for miniscrew failure. Additionally, Park et al11 found that mobility, right side of jaw the mandible and inflammation are among 17 clinical variables in microimplant failure.
CONCLUSION
The concept of TADs is a relatively new application of more established clinical methodologies. Although the clinician can look to the literature for answers, much is still unknown and will require future prospective basic science and clinical studies. The future development of TADs for orthodontic anchorage will establish a more complete understanding of the biology associated with both oseointegrated and nonintegrated devices.
The mini screw system used for anchorage gives the orthodontist another tool to approach a most difficult problem confronting us on a daily clinical basis.
Microimplants can provide absolute anchorage for the movement of whole dentition, as well as the movement of one or two teeth for prosthetic needs. It simplifies treatment mechanics by eliminating reactive mechanics.
REFERENCES
1. Mini-implants in Orthodontics: Innovative anchorage concepts- Quintessence Publishing Co Ltd; Dr. Björn Ludwig,Dr. Sebastian Baumgaertel , Dr. S. Jay Bowman.
2. The use of temporary anchorage devices for molar intrusion: J Am Dent Assoc, Vol 138, No 1, 56-64.2007; Neal D. Kravitz, DMD, Budi Kusnoto, DDS, MS, T. Peter Tsay, DDS, PhD and William F. Hohlt, DDS.
3. Temporary anchorage devices in orthodontics: Ravindra Nanda2009, Mosby (St. Louis, Mo).
4. Seminars in Orthodontics, Volume 11, Issue 1, Pages 3-9, March 2005: Jason B. Cope.
5. Block MS, Hoffman DR: A new device for Absolute anchorage for orthodontics, AJO 107(3):251-258, 1935
6. Kuroda Sugawara Y, Deguchi T, et al : Clinical uses of miniscrew implants as orthodontic anchorage: Success rates of post operative discomfort, AJO 131(1): 9-15,2001
7. Park HS, Kim JB: The use of titanium microscrew implants as orthodontic anchorage, Keimyung Med J 18: 509-515,1999
8. Park HS: Clinical study on success rates of microscrew implants for orthodontic anchorage, Korean J Orthod 33: 151-156, 2003.
9. Miyawaki S, Koyama I , Inoue M, et al: Factors associated with the stability of titanium screws placed in the posterior region for orthodontic anchorage, Am J Orthod Dentofacial Orthop 124 : 373-378, 2003.
10 Cheng SJ , Tseng IY , Lee JJ, Kok SH : A prospective study of risk factors associated with failure of mini implants used for orthodontic anchorage, Int J Oral maxillofac implants 19 : 100-106 , 2004
11. Park HS , Jeong SH, Kwon OH:Factors affecting the clinical success of mini-or microscrew implants used as orthodontic anchorage, Am J Orthod Dentofacial Orthop 130: 18-25, 2006. |