Introduction
Oral health and obesity are directly related to diet and nutrition. Food provides us not only energy but sufficient nutrients i.e water, carbohydrates, fats, proteins, vitamins and minerals which are important for growth, maintenance and repair of our body. Besides it provides security, pleasure and means to socialise, develop rapport and friendship and to get over unpleasant emotional situation. The choice of food is affected by family income, tradition, social pressure, daily schedules, lifestyles, past and personal experiences. All these jointly create once food habits.1
Food is anything eaten, drunk or absorbed for the maintenance of life, growth and repair of tissues.
Diet is the total oral intake of a substance that provides nourishment and energy.
Nutrition, according to Dr. Nizel is a science that deals with the study of nutrients & foods, their effects on nature & function of organism under varied conditions of age, health & disease.
Nutrition according to WHO, is the science of food and its relationship to health. It is concerned primarily with the part played by nutrients in body growth, development and maintenance.
If you live for sixty five years or longer you will have consumed more than 70,000 meals and your remarkable body would have disposed off fifty tons of food. The foods you choose have cumulative effect on your body.2 During preeruptive period food exerts nutritional (systemic) effect on deciduous as well as permanent teeth affecting formation of dental matrix and its mineralization. However, during post eruptive period the food has a dietary topical effect on teeth.3
Breast milk offers unsurpassed protection against infection. This protection includes antiviral, antibacterial agents and infection inhibitors. Proper early feeding of an infant lays a foundation for lifelong eating habits. It is desirable to foster preferences that will support normal development throughout life and that may help to ward off common lifestyle diseases.
As dental caries is a dietobacterial disease, so the dentist has to consider the emotional make up, habits and daily activities for controlling and preventing dental caries. Dentists should give dietary advice including reduction of non milk extrinsic sugar consumption as an important part of their health education to their patients.4
In order to succeed in this endeavor, the dentist has to deal with dental caries as a social as well as pathological disease. Previous caries triad has been transformed in to four circles showing dental caries results from interaction between susceptible tooth, cariogenic bacteria, dietary fermentable carbohydrates and time. On the other hand consider these circles for genetics, human behavior, socioeconomic status, culture and environmental factors that lead to dental caries. An attempt needs to be made to control all these influences.
In order to influence and bring about meaningful behavior modification in individual’s food habits, the dentist has to follow one route i.e. personalized one to one nutrition counseling service with both patient and caretaker / mother / homemaker / guardian present together at the counseling session so as to highlight :
1. Recent knowledge regarding cariogenic and cariostatic nutrients, foods and food practices.
2. The method of recognizing and dealing with ‘why’ of diet.
3. The practical step by step office procedure for applying this information in a personalized diet counseling service.5
Cariogenic Foods & Practices
Sufficient scientific evidence is available to prove that the nutrient sugar in the refined or natural form is the “arch criminal” in dental caries.
The consumption of sugar & sugar sweetened food has increased steadily from generation to generation especially in the so called civilized affluent people. Values and priorities are fast changing as far as diet and eating habits are concerned.
We are moving towards convenience and snack foods in order to cope with our daily schedules, eating readily available, inexpensive and sugar rich “naked calorie” foods.
Sucrose And Dental Caries
Dental caries occurs when demineralising agents such as acid producing plaque acting on tooth enamel overwhelmed the buffering capacity and remineralisation ability of oral and dental environment.
Sucrose plays following roles in the dental caries formation.
1. It promotes growth and development of cariogenic bacterial microorganisms.
2. An ordinary amount of sucrose is the source of organic acids that causes demineralization of enamel lamellae and dentinal tubules.
3. Excess sucrose is the source of stored polysaccharide dextran, which makes plaque gelatinous and sticky and can be used as source of energy for the dental bacteria, when simple sugars are not available.
Major food factors which provide media for proliferation of cariogenic bacteria S. Mutans are carbohydrates both monosaccharides and disaccharides and foods containing even small amounts of sugars. The frequency of consumption and physical form of sugar are important influences in caries development.
Indian style sweets like pera, ladoos are less cariogenic like chocolates and toffees. The reasons are as follows:
1. In Indian style sweets the sugar particles are covered by a thin layer of fat. The sugar is not immediately available over the tooth surface to the microorganisms. By the time the covering layer of fat is dissolved by saliva, the sugar particles pass the tooth surfaces and reach the oesophagus or stomach. Therefore the sugar is not readily available over the tooth surfaces to the microorganisms for producing acids by fermentation.
2. In Indian sweets sugar particles are coarse and rough in comparison to western sweets. Being coarse and rough they do not stick to the tooth surface. In chocolates and toffees the sugar particles are much finer which easily stick on the tooth surface. Sugar particles of western sweets are available for a longer period on the tooth surface and are more cariogenic.6
Sucrose Versus Glucose Or Fructose
A frequent question is 'can sucrose be substituted for a less cariogenic, nutritive sweetening agent? There is no evidence that sucrose, glucose or fructose is noncariogenic. However reports are xylitol is least cariogenic of all the sugars.3 Cariogenicity of simple sugars if compared with starch shows that starch is less cariogenic than sugar.
Fluorides And Proteins
Fluorides in water or otherwise have strong anticaries effect and protein rich diet too exerts anticaries effect.
Protein rich diets are high in phosphates which contribute significantly to lessen caries incidence.
Eating Habits And Food Consistency In Dental Caries
The major eating habits which need attention are:
1. The frequency of between meals snacking.
2. Physical form and retentiveness of sugar sweetened snacks on and between teeth.
3. The amount of sugar added to food or beverage for sweetening.
It is the length of intimate contact of fermentable carbohydrates with plaque bacteria which determines its cariogenic potential.
If one considers dental caries to be the result of imbalance between remineralisation and demineralisation, keeping the interface between enamel surface and dental plaque exposed to continuous low pH environment will increase caries initiation.
Nonretentive (liquids) sucrose containing foods consumed between meals lowers pH of saliva.
The more retentive adherent sweets, the longer period of acid contact with enamel surface. On the other hand, firm, detersive and nonretentive foods will stimulate salivary flow thus increasing the buffering capacity of oral environment so that local acid production adjacent to enamel surface can be neutralized.7
“Why” Of The Diet
Why means determining the reasons for food selection and food habits, knowing factors which motivate the individuals to eat or not eat sweets. It is important for making the diet prescription acceptable and implementable for continued use, to know the reasons for poor selection of diet whether lack of knowledge, funds or psychological stress or systemic condition or some illness or medication. To extract this information, indirect counseling like patient volunteering about his daily routine is done.
General areas required to be known are daily routine in regular, or vacations, economic status, ethnic eating habits, any food allergy, medical problem or adolescent growth spurt to ascertain reasons for food selection. Excessive nibbling is sometimes due to psychological stress, anxiety, depression, guilt, parental rejection, sibling rivalry or domestic discord.
Success and failure of counseling will depend upon motivation of the individual to co-operate which can be achieved by
1) Explaining the nature and consequences of the problems so that the individual understands its relevance with the role of food in etiology of problem.
2) Providing opportunity for the individual to find his/her own solution and encourage them to actively analyze the cariogenicity and adequacy of his diet.
3) Arranging conditions to engage the person in desired behavior, to let him choose his own diet based upon the fact that he knows what is right and what is wrong, reinforcing his choice by approval and commendation.
4) It is helpful to appeal to adolescent's esthetic sense, improvised look and better performance in school.
5) Ways can be suggested to keep him busy so that there is no time left for snacking.
Personalised Diet Counselling - Where?
Counselling session should be done in the privacy of a consultation or patient education room and never in the operatory, as fear of dental instruments should be avoided. The atmosphere should be comfortable and relaxed.
Who Should Counsel?
The best qualified person is the Dentist as he/she knows all about nutrition and is an authority figure so will get more cooperation from the patient. If it's not possible for the dentist to do the counselling then dental hygienist or dietician who has some knowledge about oral health sciences and oral pathology would be acceptable. The person counselling should be able to answer all the questions regarding food, nutrition and dental health.
How does one communicate best?
The counselling should be nondirective. Let the patient be guided to right answers and make his own decisions. Seeing the feasibility and practibility encourage the patient to be involved. It will be possible through:
1. Using soft sell approach.
2. Treating the patient with respect.
3. Seeking his/her opinion rather than forcing upon him something, let the patient bear the responsibility for making change.
4. Not making issue of negative aspect but commending the positive ones.
5. Guiding the individual to write his own prescription.
6. Providing enough suitable alternatives.
What is counseling procedure?
Diet counseling to be meaningful to patient and expedient to the counselor should be done in an ordered and organized fashion. Different steps followed are
1. A simple initial screening of patient that shows 24 hour food intake which will simply disclose excesses, inadequacies and potential cariogenicity of the individual's diet.
2. Obtain a representative food intake pattern by simply asking the patient to keep a five day food diary preferably including a weekend. This gives a general idea of his food habits.
3. An average might serve as a record of patient's typical food habits. Explain to the patient that the success of the programme like any other depends mainly on his cooperation. In order to get his cooperation, you must know about his lifestyle, daily routine, past medical and dental history.
4. Determine the why of his diet by asking him/her to recount a typical day's routine, from the time he gets up in the morning till he goes to bed at night. Gather information about not only his personal likes and dislikes but about his habits, family relationships, way of life, family's dental health, food habits and his medical history. Record his spare time activities and snacking. Special consideration is given to the patient's concern regarding bad breath, taking alkalizing medication and use of marijuana and narcotics.
5. Explain the nature of dental decay, the factors involved in its initiation and extension by following diagram (Figure 1)
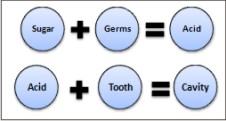 | Figure 1 - Factors Involved In Initiation And Extension Of Dental Decay
 |
Once it's clear to the patient that sugar is the arch criminal in caries process it is logical to discuss his food diary and let him circle in red, all the sugar sweetened solids and liquids in his food diary. He/ she will be surprised to know how many sweets have been eaten by him. Still more striking will be calculating the total number of minutes of acid to which teeth will be exposed in a day.
This will be given by the number of total sweet exposures multiplied by twenty. The patient will be simply surprised and guilty, if you ask the patient what do you think if your tooth is attacked by acid for one or two hours per day.
Don't be punitive or dramatizing about excessive use of sweets, as the patient will know his mistakes by now and would like to improve upon too. At this stage determine the nutritional adequacy of his/ her diet, which is done by comparing the actual food intake with the daily recommended allowances expressed as about (Figure 2).
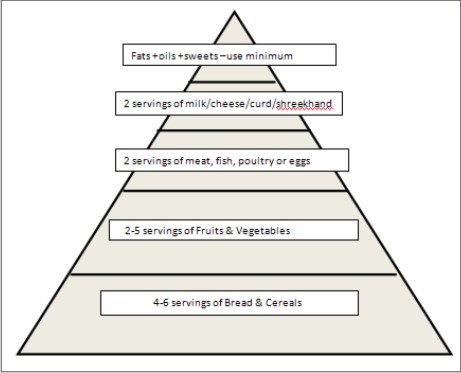 | Figure 2 - Food Guide Pyramid
|
In terms of number of sugar exposures and nutritional adequacy. He will be pleased to know that he became able to prescribe himself an acceptable meal plan which is nutritious as well as low in carcinogenicity. Follow up is important for reinforcing the modified behavior as it is important for any other home care programme for plaque control. Encouragement and removing misunderstandings during future appointments is very important.
Instructions
1. Please record in detail everything you eat or drink in the order in which it is eaten.
2. The frequency of eating is an important consideration; therefore, include between meal snacks like toffees, chewing gum, sweets etc.
3. The following information is essential:
a) The amount in household measurements such as 1 cup, 1 teaspoon, ½ glass, 1 serving
b) The addition of sugar or sweetened syrup/powder (Bournvita/Complan) to milk or other foods such as 1 bowl of cornflakes with ½ glass milk and 2 tsp sugar
4. Example:
Conclusion
Since dental caries is a dietobacterial disease, improving patient's nutrition just as much as preventing plaque accumulation, should be a part and parcel of total preventive dentistry service. For a dentist it's very important to use this basic information meaningfully in his/her practice. This can be done in an ordered and organized manner. Nutrition counseling will definitely be successful if it is done with conviction and due importance to what and why of diet is given.
 | Five Day Diet Diary Chart
|
References
1. Teresa A. Marshall. Diet and nutrition in pediatric dentistry. Dental Clinics of North America 2003; 47:279-303.
2. Sizer F, Whitney E. Nutrition concepts and controversies. 8th edition Wadsworth; Belmont; 2000 p. 2.
3. Nizel AE, Papas AS. Dietary counseling for the prevention and control of dental caries. Nutrition in clinical dentistry. 3rd edition WB Saunders: Philadelphia; 1989. P. 277-308.
4. Morgan MZ, McFarlane E, Stewart KF, Hunter ML and Fairchild RM. An assessment of nutritional information in oral health education leaflets. Community Dental Health 2010; 27:81-88.
5. Nizel AE. Personalized Nutrition Counseling. J Dent Child 1972; 39:353-360, September-October.
6. Chandra S, Chandra S. Textbook of Preventive Dentistry.1st edition Jaypee: Newdelhi ; 1999. P. 65-66.
7. Tondon S. Textbook of Pedodontics. 2nd edition Paras Publication: 2008. P. 225
8. Scheinin A, Makinen KK: Turku Sugar studies, Acta Odontol Scand, 1987 70; 33:1.
9. Kulkarni SS, Deshpande SD. Caries prevelance and treatment needs in 11-15 year old children of Belgaun city. J Indian Soc Pedo Prve dent 2002; 20:12-15.
10. Sahoo PK, Tewari A, Chawla HS, Sachdev V. Interrelationship between sugar and dental caries- a study in child population of Orissa. J Indian Soc Pedo Prve dent 1992; 10:37-44.
11. Shaw JH, Krumins I, Gibbons RJ. Comparison of sucrose, Lactose, Maltose and Glucose in the causation of Experimental oral disease. Arch Oral Biology 1967; 12:755-768.
12. Newburn E. Sucrose, the Arch Criminal Of Dental Caries. J Dent Child 1969; 36:239-248, July-August. |