Introduction:
The separation of instruments during endodontic therapy is a troublesome incident and ranges from 2-6% of the cases investigated.1 The most common causes for file separation are improper use, limitations in physical properties, inadequate access, root canal anatomy, and possibly manufacturing defects.2 Instrument fractures during root canal treatment hinder the clinician from optimal preparation and obturation of the entire root canal system. This affects the long term prognosis of root canal treatment negatively.3,4 When instrument separation occurs, the clinician has the choice of leaving the instrument in the canal or attempting to remove it either surgically or nonsurgically.5
The removal of separated instruments from the root canal in most cases is difficult and at times impossible.6 Numerous methods have been proposed to remove obstructions from within the root canal, with varying degrees of success.7-10 This case report is about the successful retrieval of a separated file from maxillary left central incisor using a Tube-and-Hedstrom file technique.11 This is a readily available, easy to practice, cost effective method to retrieve separated instrument and requires no special equipment.
Case Report
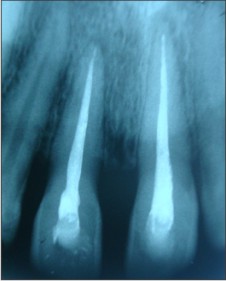
A 25 year-old female patient reported to Department of Conservative Dentistry & Endodontics with pain in upper front teeth for which root canal treatment (RCT) was done a month back in private clinic. The maxillary left central incisor was sensitive to percussion and palpation. The radiograph revealed two separated H-files in maxillary left central incisor, one extending from approximately 1 mm below the access to the radiographic apex and other extending from CEJ till the junction of apical and middle third of root. Radiograph also showed incompletely obturated maxillary right central incisor (Fig 1).
 | Fig 1 : Preoperative photograph.
 |
Retreatment was planned for both maxillary right and left central incisor. The hollow tube method was used to remove the seprated files from maxillary left central incisor. Rubber dam was applied (Hygiene, Coltene). High-speed tapered fissure bur was selected to create straight-line access to canal orifice and also remove the previously filled material from the pulp chamber.Canal was pre-enlarged with Gates Glidden drills #3 or #4 (Dentsply Maillefer; Tulsa) to maximize visibility coronal to the obstruction. After having prepared a straight line access, the coronal end of the separated file was readily visible with the microscope. Visualization of the obstruction is very important during the fragment retrieval process because it will allow better control of dentin removal, ensuring centering within the canal and positioning of the ultrasonic tip alongside the fractured instrument. A 1- to 2-mm deep circular groove was prepared around the coronal end of the separated instrument using ultrasonic scaler tip (BS-1) to obtain a space between the instrument and the canal walls. With this procedure, the periphery of the file was successfully exposed and was gripped with the cut piece of stainless-steel tubing/canula (supplied with EDTA gel syringe) pushed over the exposed end of the broken file (Fig 2). Subsequently, a piece of A Hedstrom No. 55 file (size depends on the diameters of the needle and the separated instrument) was pushed using a clockwise rotation mode through the tubing passing beyond the tip of the separated instrument, and alongside it until the Hedstrom file cannot progress any further. At this point, a very tight connection is usually formed between the Hedstrom file, needle, and separated instrument. Artery forceps was used to grasp the needle and pull the fractured file out in a twist turn motion (Fig 3, 4).
 | Fig 2 : Stainless steel tubing used to grip the separated file.
|
 | Fig 3 : Artery forceps used to grasp tubing and remove the separated file.
|
 | Fig 4 : Tight connection formed between H-file, tubing and separated file.
|
Radiograph revealed the second separated file extending from CEJ till the radiographic apex, lying adjacent to mesial wall of the canal (Fig 5). Ultrasonic scaler BS-1 tip was used to obtain space between the instrument and the canal walls. The removal of the second separated instrument was done similarly, under the microscope using the previously described method (Fig 6). Working length was determined using IOPA X-ray for both 11 & 21 followed by cleaning & shaping. All instrumentation was accompanied by copious irrigation with 5% sodium hypochlorite. An intra canal dressing of commercially available calcium hydroxide was given. A sterile cotton pellet was placed in the pulp chamber and the access cavity was double sealed with an intermediate restorative material (IRM, Dentsply). At the next appointment after 7 days, the patient was asymptomatic and the canal was obturated with laterally condensed gutta percha using Acroseal sealer (Septodont), and the root canal opening was sealed using composite material (Synergy D6,Coltene) (Fig 7).
 | Fig 5 : Second separated file seen in maxillary left central incisor.
|
 | Fig 6 : Both separated files removed from maxillary left central incisor.
|
 | Fig 7 : Post- Operative Photograph.
|
Discussion
Intracanal separation of instruments usually prevents access to the apex, impedes thorough cleaning and shaping of the root canal, and thus may compromise the outcome of endodontic treatment and reduce the chances of successful retreatment.8,9 In such cases, prognosis following an endodontic therapy depends on the condition of the root canal (vital or nonvital), tooth (symptomatic or asymptomatic, with or without periapical pathology), level of cleaning and shaping at the time of separation, the level of separation in the canal; and is generally lower than that with normal endodontic treatment.1,12
Success of nonsurgical fractured instrument removal from root canals depends on the canal anatomy, the location of the fragment in the canal, the length of the separated fragment, the diameter and curvature of the canal itself, and the impaction of the instrument fragment into the canal wall.2 Instruments located in the straight portions of the canal can usually be removed.The chances of success should be balanced against potential complications. As a rule of thumb, if one-third of the overall length of an obstruction can be exposed, it can usually be removed.13 Despite all that has been reported, the previous enlargement of the dentin walls is essential for the capture of the instrument.14,15 Roig-Greene (1983) also reported that the tip of the object must be free in the center of the canal, far away from the canal dentin walls.16
Traditionally, retrieving broken instruments posed formidable challenges. One time-honored technique has been the use of small files to either remove, or at least bypass, the broken instrument.13 Over time retrieval techniques evolved, i.e., Canal Finder system, Masserman Kit, Endo Extractor System, Ultrasonics, and several kinds of pliers but were often ineffective because of limited vision and/or restricted space. The endo extractor technique using cyanoacrylate and a steel tube or cut needle, often contaminates the canal walls with adhesive.17,18 On the other hand, retrieval of obstructions using Masserann instruments requires a large access canal, with a diameter of at least 1.2 mm to be prepared.19 Such procedures have a high risk of perforating the root. The braiding technique is less effective, because there is no constant tight bonding to the separated instrument.20 At present, there is not any standardized procedure for safe and consistently successful removal.21 Also various technique and retrieval kits discussed above are either expensive or not easily available to the clinician.
This article describes an indigenous method, a Tube-and-Hedstrom file technique that was used for retrieval of two separated instruments from maxillary central incisor. Canal was pre-enlarged with Gates Glidden drills #3 or #4 (Dentsply Maillefer; Tulsa) to maximize visibility coronal to the obstruction. When the fractured instrument is below the canal orifice, one basic method for removal of this fragment requires the exposure of approximately 2 mm of the separated fragment.22 This allows a device to be used to get purchase on it and retrieve it. A 2 mm deep circular groove was prepared with an ultrasonic scaler tip (BS-1) circumferential to the coronal end of the broken file, under the microscope. The enhanced vision with magnification and illumination from a microscope allows clinicians to observe the most coronal aspects of broken instruments and to remove them without any perforations.11,23 With this procedure, the periphery of the file was successfully exposed. However, the file was very tightly wedged into the dentin and efforts to loosen the file with manual pressure were unsuccessful. The hollow tube method of file removal involved sizing and gauging the correct microtube so it could reach, and be placed over, the ultrasonically exposed obstruction. In this case, needle/canula (commonly used for dispensing EDTA gel) was broken at hub level and this hollow tube acts like a micro tube to grasp the fractured file at one end and H- file is snugly inserted at the other end. It is a readily available, cost effective microtube and mild angulation in the canula allows easy accessibility. Because of the unique ability to engage, an H-file was selected and inserted into the coronal-most aspect of the microtube. The Hedstrom was then passed down the length of the tube until it was engaged tightly between the obstruction and the internal lumen of the microtube. It holds the broken instrument in tube as a wedge. This junction can easily be taken out from root canal or pulled with help of artery forceps. The removal of the second separated instrument was done similarly, under the microscope using the above described method. However, it needs frequent radiographic monitoring. It has limited application in teeth with thin and curved roots. However, Tube-and-Hedstrom file-Technique may result in easier and more controlled removal of fractured instruments from anterior teeth having thick, straight roots and although limited by space, this removal method could, at times, successfully retrieve obstructions from larger canals in posterior teeth.
Conclusion
Files lodged in the coronal and middle thirds of the root can consistently be removed without major complications. The Tube-and-Hedstrom file-Technique described here is a conservative, safe and plausible technique in cases, particularly those where tightly wedged broken instruments exist in a readily accessible position. Ample light and magnification as provided by the operating microscope is essential in the retrieval of separated instruments
References
1. Arcangelo CM, Varvara G, Fazio PD. Broken instrument removal-two cases. J Endod 2000; 26:568-70.
2. Roda RS, Gettleman BH. Nonsurgical retreatment. In: Roda RS, Gettleman BH, editors. Pathways of the pulp. 9th ed. St. Louis: CV Mosby; 2006. pp. 982-90.
3. Sjögren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod 1990; 16:498-504.
4. Sigueira JF. Aetiology of root canal treatment failure: why well-treated teeth can fail. Int Endod J 2001; 34:1-10.
5. Saunders JL, Eleazer PD, Zhang P, Michalek S. Effect of a separated instrument on bacterial penetration of obturated root canals. J Endod 2004;30(3):177-9.
6. Hulsmann M, Schinkel I. Influence of several factors on the success or failure of removal of fractured instruments from the root canal. Endod Dent Traumatol 1999; 15: 252-8.
7. Fors UG, Berg JO. A method for the removal of broken endodontic instruments from root canals. J Endod 1983; 9:156 -9.
8. Hülsmann M. Methods for removing metal obstructions from the root canal. Endod Dent Traumatol 1993; 9:223-7.
9. Okiji T.Modified usage of the Masserann kit for removing intracanal broken instruments. J Endod 2003; 29:466 -7.
10. Nehme W. A new approach for the retrieval of broken instruments. J Endod 1999; 25:633-5.
11. Suter B. A new method for retrieving silver points and separated instruments from root canals. J Endod1998; 24(6), 446-8.
12. Ward JR, Parashos P. Messer H.H. Evaluation of an ultrasonic technique to remove fractured rotary Nickel - Titanium Endodontic instruments from root canals: clinical cases. J Endod 2003; 29: 764-7.
13. Ruddle CJ. Broken instrument removal. The endodontic challenge. Dent Today 2002; 21:70 -2.
14. Fors UGH, Berg JO: A method for the removal of broken endodontic instruments from root canals. J Endod 1983; 9: 156-9.
15. Spriggs K, Gentleman B, Messer HH: Evaluation of a new method for silver points removal. J Endod 1990; 16: 335-8.
16. Roig-Greene JL. The retrieval of foreign objects from root canals: a simple aid. J Endod1983; 9: 394-7.
17. Johnson WB, Beatty RG. Clinical technique for removal of root canal obstructions. J Am Dent Assoc 1988; 117: 473-6.
18. Gettleman BH, Spriggs KA, El Deeb ME, Messer HH. Removal of canal obstruction with endo extractor.J Endod 1991; 17:608-11.
19. Masserann J.Entfernen metallischer fragmente aus wurzelkanalen.J Br Endod Soc1971;5: 55-9 as quoted in Suter B. A new method for retrieving silver points and separated instruments from root canals. J Endod1998, 24(6), 446-48.
20. Hülsmann M,Wieger R.Die Revision Von Wurzelkanalbehandlungen.Part II. Endodontie 1994; 2:115-29.
21. Nimet Gencoglu, Dilek Helvacioglu. Comparison of the different techniques to remove fractured endodontic instruments from root canal systems. Eur J Dent. 2009 April; 3(2): 90-95.
22. Terauch Y, Le O'Leary, Hideaki Suda. Removal of Separated Files from Root Canals with a New File-removal System: Case Reports. J Endod 2006;32: 789 -97.
23. Khayat BG. The use of magnification in endodontic therapy: the operating microscope. Pract Periodontics Aesthet Dent 1998; 10:137-44. |