Introduction
The Central Giant Cell Granuloma (CGCG), first described by Jaffe in 1953, is a benign lesion that usually occurs in the mandible and the maxilla1. They are usually a non-neoplastic bone lesion accounting for fewer than 7% of all benign tumors of the jaws2,3 The World Health Organization defined them as an intraosseous lesion consisting of cellular fibrous tissue containing multiple foci of hemorrhage, aggregations of multinucleated giant cells and occasionally, trabeculae of woven bone10. CGCG of the jaws mainly occurs in children or in young adults, with a predilection for females3,5. It is more common in the mandible than in the maxilla3,5, and can be confined to the tooth-bearing areas of the jaws. CGCGs can also affect extragnathic bones, mainly in the craniofacial region, and small long bones such as those of the hands and feet. The radiologic features of the CGCG comprise a unilocular or a multilocular radiolucency and varying degrees of expansion of the cortical plates. Various treatment modalities have been suggested for CGCG. The most often applied are thorough simple curettage, curettage with peripheral ostectomy, and enbloc resection.8,9 However, recurrence rates are high, ranging from 11% to 72% in different studies6.The case reported here presented with a giant cell lesion that involved the left maxilla.
Case Report
A 24 year old female was referred to Department Of Oral Pathology , Vasantdada Patil Dental College & Hospital after complaining and seeking treatment for a painless and gradual swelling in her left maxilla which was there since more than 3 month. Symptoms noted were swelling in her upper left cheek region, left buccal vestibule & palate. Swelling was reported to be insidious in onset & progressed slowly from small lesion to present size. She was in her second trimester of pregnancy. Extraoral examination revealed a diffuse swelling on the left side of face resulting facial asymmetry [Fig. 1-2].
 | Figure 1 : Extraoral view showing diffuse swelling over left side of face resulting in facial asymmetry.
 |
 | Figure 2 : Lateral view of face showing diffuse swelling over left side of face.
|
Intra-oral examination showed a swelling in buccal aspect extending in relation to upper left 4-5-6-7-8 teeth. There was also expansion of the palate [Fig. 3].
 | Figure 3 : Intraoral view showing swelling over palate
|
It had a smooth surface with no evidence of fluctuation on palpation. It was non tender & hard on palpation. The teeth showed grade1mobility. A PNS view [Fig. 4] and a computed tomography scan (CT) [Fig. 5-6] revealed a soft tissue mass seen completely obliterating the left maxillary antrum with thinning and destruction of parts of the wall. The mass extended inferiorly into the body of the maxilla upto alveolus, involving the teeth. Infero-medially, it reached the midline of the maxilla. Medially, it almost obliterated the posterior third of the left nasal cavity. Posteriorly it reached the lateral and medial pterygoid plates. Superiorly it extended up to the floor of the orbit. It shows diffuse radiolucency and varying degrees of expansion of the cortical plates. Histological examination shows clusters of relatively sparse and randomly scattered multinucleated giant cells embedded in a stroma of spindle-shaped mononuclear cells [Fig. 7-8]. Theses findings were consistent with diagnosis of CGCG. It is difficult to distinguish with brown tumor of hyperthyroidism. Hence,serum levels of calcium & alkaline phophatase were adviced and found out to be in normal limits.
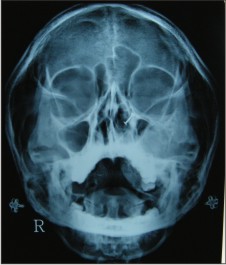 | Figure 4 : Paranasal view showing involvement of left maxillary sinus.
|
 | Figure 5 : Coronal CT showing an expansile lesion arising from inferior aspect of left maxilla with destruction of floor of sinus .
|
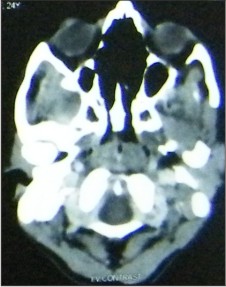 | Figure 6 : Axial CT showing well defined radiolucency.
|
![Figure 7 : Low power photomicrograph of CGCG showing clusters of relatively sparse and randomly scattered multinucleated giant cells embedded in a stroma of spindle-shaped mononuclear cells[H\E, 10X magnification]](article-image-1456-FIGURE_7_LOW_POWER_PHOTOMICROGRAPH_OF_CGCG_SHOWING.jpg) | Figure 7 : Low power photomicrograph of CGCG showing clusters of relatively sparse and randomly scattered multinucleated giant cells embedded in a stroma of spindle-shaped mononuclear cells[H\E, 10X magnification]
|
![Figure 8 : High power photomicrograph of CGCG showing multinucleated giant cells.[H\E, 40X magnification]](article-image-1457-FIGURE_8_HIGH_POWER_PHOTOMICROGRAPH_OF_CGCG_SHOWIN.jpg) | Figure 8 : High power photomicrograph of CGCG showing multinucleated giant cells.[H\E, 40X magnification]
|
Local injections of corticosteroid for a period of 4 weeks was given as there were no improvement in condition patient undervent for surgical removal of lesion.
Discussion
Central Giant Cell lesions of jaws are uncommon8. It can occur at any age but presents most frequently in the 2nd and 3rd decades5 and involves the mandible more than the maxilla. It is twice as frequent in females7. Usually it is only a painless swelling, but growth in some cases is so rapid and the mass can also rarely erode through bone particularly of the alveolar ridge to produce a soft tissue swelling 7. Although lesion is expansive and invasive, it does not usually involve perinueral sheets, for this reason parasthesia is usually not observed in these patients. Trauma has been considered as an important etiologic factor in the initiation of this lesion9.Association of t (X;4) (q22; q31.3) in the etiology of giant cell granuloma has been reported10. The clinical behaviour of GCG ranges from a slowly growing asymptomatic swelling to an aggressive lesion. When GCG is a slow-growing lesion, it can be asymptomatic and discovered on a routine X-ray, while the rapidly expanding, aggressive variety is characterized by pain and facial swelling3.These fast growing lesions also have a high rate of recurrence. It has been reported that recurrence is usually found when the lesion perforates the cortical plates to involve the surrounding soft tissue11. Radiologic features vary from undefined destructive lesions to a well-defined, multilocular appearance. Teeth or roots displacement are the most consistent features which are clearer on CT than on plain film . However, none of these radiological features is specific for CGCG13 Histologically, multinucleated giant cells, in a cellular vascular stroma, and often new bone formations are detected. The osteoclast-like giant cells have a patchy distribution and are usually associated with areas of haemorrhage. Ultrastructurally, the proliferating cells include spindle-shaped fibroblasts, myofibroblasts, and inflammatory mononuclear cells. GCG is a vasculararized lesion that shares many features with the aneurysmal bone cyst. Differentiation from the latter can also be difficult histologically. However, the aneurysmal bone cyst is characteristically composed of honeycomb blood-filled spaces with a lining of flat non-endothelial cells. Brown tumour of hyperparathyroidism is histologically very similar to GCG. Thus, all patients with suspected GCG, should have serum calcium, phosphate and alkaline phosphatase levels evaluated, to exclude the possibility of hyperparathyroidism.The non-ossifying fibroma is histologically very similar to the GCG which can, however, be differentiated from the latter since the granuloma-like aggregate of giant cells and the fibrous stroma found in GCG, are not typical features of non-ossifying fibroma. There is always matter of speculation between GCG & Giant Cell Tumor[GCT] .GCT occurs predominantly in long bone & rarely in jaw bones. They are usually painful & fast growing .In 10%, pathologic fracture is first sign. Microscopically, GCT shows background of mononuclear cells which are rounded and polygonal in shape. There are greater number of nuclei of giant cell with no vascularization & blood spaces8 .In cases of Cherubism, two or more jaw quadrants contain lesions histologically similar to giant cell granuloma. The disease occurs in young children, often with a history of other afflicted family members.Cherubism also found to regress its own & no surgical treatment required12. Although most GCGs in the jaws are treated readily by curettage, a minority pose problems sometimes benign GCG can prove difficult to treat either because of its large size, the difficulty of extensive curettage in the fragile facial bones, or because of the risk to facial growth centers and developing teeth. A particular problem is the extremely rapid and destructive growth of GCG during pregnancy. Medical treatment of GCG has proved successful. Intralesional steroid injections result in growth arrest and even resolution of the lesion, and this simple and inexpensive treatment may avoid surgery. Harris first proposed Administration of calcitonin for treatment of CGCG14. Biphosphonates have been administered intravenously in CGCG with promising results9.
Conclusion
Central Giant Cell Granuloma is rare disease & its occurrence in maxilla is not common.
The clinical behavior of this lesion is quite variable & difficult to predict . Hence, it is suggested to consider it in differential diagnosis of swelling of maxillary posterior region. It's occurrence in pregnancy was also reported to be uncommon.
References
1. Jaffe HL. Giant-cell reparative granuloma, traumatic bone cyst,and fibrous (fibro-osseous) dysplasia of the jawbones. Oral Surg 1953;6:159-75.
2. Kurtz M, Mesa M, Alberto P. Treatment of a giant cell lesion of the mandible with intralesional glucocorticosteroids. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;91:636-7
3. Birgit Kruse-Losler, Raihanatou Diallo. Central giant cell granuloma of the jaws: A clinical, radiologic,and histopathologic study of 26 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;101:346-54
4. Kramer IRH, Pindborg JJ, Shear M, editors. Histological typing of odontogenic tumours. 2nd ed. Berlin: Springer-Verlag; 1991.p. 31.
5. Shafer's Textbook of Oral Pathology,Fifth Edition
6. Dror M. Allon, DMD,a Yakir Anavi, Central giant cell lesion of the jaw: Nonsurgical treatment with calcitonin nasal spray. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;107:811-818
7. Cawson RA, Odell EW, Cawson's Essentials of Oral Medicine and Pathology, 7th ed, Churchill Livingstone;2002. p.135-136.
8. Roderick A. Cawson , William H. Binnie, Lucas's Pathology of Tumors of the Oral Tissue.5th Ed,p.174
9. Amar A Sholapurkar, Keerthilatha M Pai,Auswaf Ahsan,Central Giant Cell Granuloma of anterior Maxilla:Case Report ,Indian Journal Of Dental Research 2008:19;1;p.78-82
10. Jan de Lange, Hans P. van den Akker, Central giant cell granuloma of the jaw: a review of the literature with emphasis on therapy options .Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:603-15
11. A. Ciorba, G. Altissimi, Giant Cell Granuloma Of The Maxilla: Case Report, Acta Otorhinolaryngol Ital 24, 26-29, 2004
12. Pieter J. Slootweg ,Pathology of the Head and Neck, Springer 2006, p.124
13. Israel Kaffe, a Leon Ardekian,Radiologic features of central giant cell granuloma of the jaws, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;81:720-6
14. Esther M. O'Regan, Donald H, Rapid growth of giant cell granuloma in pregnancy treated with Calcitonin,Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2001;92:532-8.
|