Introduction:
Complete dentures are primarily mechanical devices, but since they function in the oral cavity, they must be fashioned so that they are in harmony with its surrounding to provide optimum stability, retention and comfort. Dentist and Prosthodontist encounter problems when making complete dentures for patients who have severely atrophic residual ridges. The problem is mostly seen in the mandible. Following dental extraction, alveolar bone resorbs until only basal bone remains1. Furthermore, systemic diseases such as diabetes mellitus, osteoporosis, osteosclerosis and osteomalacia can exacerbate the situation2. The advanced resorption of the mandibular residual ridge produces a flat and sometimes concave foundation, what we call “the difficult lower jaw”3, leading to reduced retention and stability.
Dental implants may provide stabilization of complete denture for the atrophic mandible, however there may be situations when it is not possible to provide implants on the grounds of medical, surgical or costs factors. The neutral zone technique is an alternative approach for these complex cases. The technique is not new but is one that is valuable and yet not often practiced4.
In 1948, Sir Wilfred Fish concluded that dentures have three surfaces (impression surface, occlusal surface, polished surface), each with its own function and important role in achieving denture retention and stability5. He also described how dentures should be constructed in the 'dead space', which later became known as the neutral zone6.
The neutral zone has been defined as the area in the mouth where during function; the outward forces of the tongue are neutralized by the inward forces of the cheeks and lips7. This definition is an over-simplification but serves to create a basic mental image of what a denture, constructed in the zone, is trying to achieve.
All oral functions such as speech, mastication, swallowing, smiling and laughing involve the synergistic actions of the tongue, lips, cheeks, and floor of mouth which are very complex and highly individual. Failure to recognize the cardinal importance of tooth position and flange form and contour often results in dentures which are unstable and unsatisfactory, even though they were skillfully designed and expertly constructed. The coordination of complete dentures with neuromuscular function is the foundation of successful stable denture8.
Teeth should be placed as dictated by the musculature. This will vary for different patients9. Positioning artificial teeth in the neutral zone achieves two objectives: First, the teeth will not interfere with the normal muscle function; and second, the forces exerted by the musculature against the denture are more favorable for stability and retention8. In addition, facial appearance is improved with improved support of the facial musculature10.
The purpose of this clinical report is to describe a simplified procedure for fabrication of a mandibular complete denture with altered denture space placed in the neutral zone using impression compound material.
Case Report:
A 65-year-old man reported to the institution for replacement of his missing teeth. A brief dental and medical history was taken. Clinical Examination included assessment of the mucosa and intra-oral palpation of all areas adjacent to potential denture peripheries. Clinical examination revealed a severely resorbed, flat mandibular alveolar ridge (Fig 1). It was decided to use the neutral zone technique for fabrication of mandibular denture.
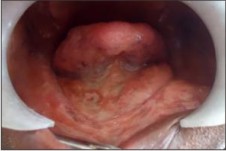 | Fig 1: Edentulous Mandibular Ridge
 |
Maxillary and mandibular preliminary impressions were made using irreversible hydrocolloid. Border molding was done with green stick impression compound and a wash impression was made with zinc oxide eugenol.
Procedure:
1. Maxillary and mandibular occlusion wax rims were fabricated so as vertical dimension of occlusion could be determined with the usual 2 - 4 mm freeway space.
2. Location of the maxillary jaw according to skull base was transferred to semiadjustable articulator (Hanau Wide-Vue Arcon Articulator, Waterpik, Fort Collins, USA) by the face bow transfer (Waterpik, Hanau Springbow).
3. The vertical dimension of occlusion and centric relation positions were recorded.
4. With guidance from the determined vertical height, both models were mounted on the articulator in centric relation position. Wax from the mandibular occlusion rim was removed.
5. Low fusing modeling compound (mixture of impression compound cake and green stick compound) was used to record the neutral zone.
6. A water bath preheated to the proper temperature is used to soften the material, which is then kneaded and worked until it is uniformly soft. The amount of compound required to make an occlusion rim is rolled and placed over the mandibular denture base made of acrylic, which was carefully adjusted in the mouth to ensure that it was not overextended and remained stable during swallowing, opening and speaking. The mandibular denture base with the softened low fusing compound was placed in the patient's mouth.
7. The patient was instructed to talk, swallow, lick, suck and then purse her lips, and drink some water several times so that right lingual and buccal surfaces of the impression were molded correctly. After 3-5 minutes, the set impression of the neutral zone was removed from the mouth and examined (Fig 2 & 3).
 | Fig 2 & 3: Neutral Zone Impression with Low Fusing impression compoundÂ
|
8. Silicone Putty indices were made around the neutral zone impression (Fig 4, 5 & 6). The neutral zone impression is then removed from the base plate and the indices were replaced. The index had preserved the space of the neutral zone.
 | Fig 4: Putty Index on Buccal Side
|
 | Fig 5: Putty Index on Lingual Side
|
 | Fig 6: Putty Index Around The Neutral Zone impression
|
9. Wax was poured into the space giving an exact representation of the neutral zone (Fig 7).
 | Fig 7: Wax Poured In Neutral Zone Space
|
10. Mandibular teeth were then set up exactly following the index. During the setting up of the teeth their position were checked by putting the indices together around the wax rim (Fig 8). Maxillary teeth were arranged with the guidance of lower teeth with esthetic rules.
 | Fig 8: Teeth Arrangement in Neutral Zone
|
11. Wax up was done after teeth arrangement and all polished surfaces in contact with tongue, cheek and lips were prepared up to the neutral zone. Wax try in was done to check the appearance and occlusion (Fig 9).
 | Fig 9: Wax Trial Denture
|
12. Finally the trial dentures were flasked and finished in the conventional manner. On final insertion the dentures were fully inspected and a check record performed to eliminate any minor occlusal errors (Fig 10).
 | Fig 10: Denture Insertion
|
The dentures with improved retention, stability and improved facial appearance were provided to the patient as they have been constructed in harmony with their surroundings.
Summary:
The neutral zone philosophy is based on the concept that for each individual patient there exists a specific area with in the denture where the function of the musculature will not unseat the denture, and at the same time where the forces generated by the tongue are neutralized by the forces generated by the lips and cheeks. The neutral zone approach with low fusing compound is a more practical and economically feasible treatment in the general dental practice for patients with atrophic mandibular ridge. It is imposible to construct a denture where the perfect, absolute equilibrium exists and no displacement occurs. However meticulous attention to detail in every phase of denture construction allowed a successful treatment.
Referances:
1. McCord JF, Smith P, Grey N. Treatment of Edentulous Patients. Ed Churchill Livingstone. Edinburgh. 2004. 32-3.
2. Zarb GA, Finer Y. Identification of Shape and Location of Arch Form: The Occlusion Rim and Recording of Trial denture Base In Zarb-Bolender (Ed).
3. Brill N, Tryde G, Cantor R. The dynamic nature of the lower denture space. J Prosthetic Dentistry 1965; 15:401-417.
4. Gahan MJ, Walmsley AD.The neutral zone impression revisited. Br Dent J 2005;198 (5):269-72.
5. Indrawati L, Kusdhany L, Soebekti TS. The neutral zone concept revisited - overcoming instability and lack of retention in complete lower denture construction. Malaysian Dent J 2009; 30(1) :49-52.
6. Fish EW. Using the muscles to stabilize the full lower denture. J Am Dent Assoc 1933; 20: 2163-9.
7. Beresin VE, Schiesser FJ. The neutral zone in complete and partial dentures. C.V. Mosby Co., 1978:p-15.
8. Beresin VE, Schiesser FJ. The neutral zone in complete dentures. J Prosthetic Dentistry 2006;95:93-100.
9. Kursoglu P, Ari N, Calikkocaoglu S. Using tissue conditioner material in neutral zone technique. NYSDJ 2007: 40-2.
10. Dawson PE. Functional Occlusion from TMJ to Smile Design. Canada. Elsevier. 2007. 131-5.
|