Introduction
Dental implant has contributed to improve quality of life for many patients over the past 20 years.1 The anterior maxillary jaw is frequently called the “esthetic zone” because of its high visibility and influence on facial appearance. Tooth loss in the anterior region is for most patients a deeply traumatic experience. Although an anterior tooth has mechanical functionality, it is the compromised facial esthetics associated with tooth loss that is the patient's primary concern2. Implant placement and single-tooth restoration in this region can present some esthetic challenges for the clinician and demanding procedure because of the region's visibility and role in smile performance.3,4 The earliest implant patients were grateful simply to recover something approaching normal masticatory function and phonetics. But as implants began to move into the clinical mainstream, patients understandably expressed a desire for more natural-looking restorations. In response, implant practitioners developed a remarkable arsenal of knowledge and technology for delivering highly aesthetic implant-supported prosthetic solutions. As this has occurred, the speed with which those restorations can be delivered has moved to the forefront of patient concerns. Alveolar ridge resorption, along with soft tissue recession by tooth loss, often results in defects that prevent the ideal implant placement and compromise the final esthetic outcome. To achieve esthetically acceptable implant restoration with the soft tissue complex that mimic the same tooth on contra lateral side in the same arch, both the hard and soft tissue defects must be restored and implant placed 2 to 5 mm from the predetermined free gingival margin.5,6 Furthermore, it needs to be within the confines of the root emergence of the final restoration.7-9 Various bone grafting and/ or soft tissue grafting procedures have been recommended to restore the proper ridge contour to allow for the ideal implant placement.10,11 Immediate implant placement has also been suggested as a means to minimize tissue resorption.12,13 Various factors may prevent re-creation of an ideal hard and soft tissue environment, thus preventing placement of implant in an ideal location and Prosthodontist encounters a unfavorable situation to achieve esthetically acceptable restoration. For optimal esthetic, function and emergence profile, the implant and abutment axis must coincide, an adequate interocclusal space must be present, and there must be a sufficient soft tissue thickness above the implant. However in reality there are clinical situations, which require the modification of the abutment. Schmitt et al, described a custom abutment system, was used to provide solution to limited interocclusal space8, poor implant angulation.14 This clinical report describes an abutment design used for esthetically unfavorably placed implants in the anterior maxilla to achieve esthetically acceptable restoration. Prosthodontic techniques that enabled this patient to have a successful outcome included the use of angulated abutment within the bulk of the prosthesis. For this patient the prosthodontic compromises were preferred over another surgical procedure with the additional time, discomfort, increased cost, and possible surgical morbidity. It is important that the patient understand the compromises and potential problems when implant placement is not ideal, especially the potential for implant failure. This technique combines a custom abutment from a hexed UCLA-type plastic burn-out pattern and a manually threaded setscrew hole is a relatively inexpensive and uncomplicated approach to eliminate problems caused by unfavorable implant inclination.
Clinical Report
A 25 year old female patient presented at dental OPD with the chief complaint, “missing single front teeth and replacement of the same for esthetic motivation.” (Fig.1). The treatment options, which included a removable partial denture (RPD), a fixed partial denture (FPD), and an implant single crown, and the advantage and disadvantage of each option were presented to the patient. The patient was opposed to the idea of wearing a removable prosthesis, and because the potential abutments were not previously restored, she expressed a preference for the implant single crown to avoid preparation of the adjacent teeth.
 | FIG. - 1 Preoperative Intraoral Photograph
 |
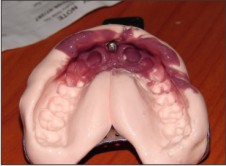
The patient was informed about the procedure and written consent was obtained. Implant height and diameter was calculated from standard periapical radiograph (Fig. 2) and Occlusal view (Fig. 3) and than implant was placed with following sterile surgical protocol (Fig. 4). At that time, temporary prosthesis was delivered (Fig.5). However, 6 month later at the time of second stage surgery, it was observed that the implant found labially and esthetically unpleasant (Fig. 6). Treatment options for restoring the dentition to optimal function and esthetics were presented to the patient. Options included removal and replacement of existing implant with appropriate grafting, or restoration with a removable partial denture over existing implant or fixed partial denture. The patient didn't want further surgical procedures to remove and replace existing implant or to graft hard and soft tissue defects, and desired a fixed prosthesis. According to patient's requirement, we planed that the implant would be restored in the present position with angulated abutment and porcelain fused metal restoration. Healing abutment was removed to reveal healthy tissues and an impression coping was placed. An implant level impression was completed with poly-vinyl polysiloxane impression material (Aquasil, Dentsply, Germeny) to record the implant position (Fig. 7). Implant analogue was placed, a gingival replica was completed in silicone material, and the definitive cast was poured in type V die stone (Kalstone, Kalabai Pvt. Ltd. Mumbai).
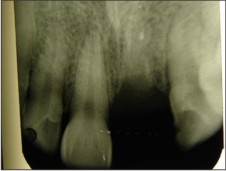 | FIG. - 2 Preoperative IOPA
|
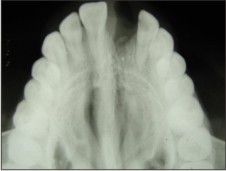 | FIG. - 3 Preoperative Occlusal Radiograph
|
 | FIG. - 4(a) Implant Placed
|
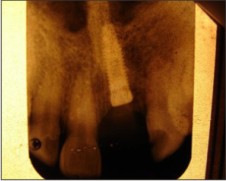 | FIG. - 4(b) IOPA After Implant Placement
|
 | FIG. - 5 TEMPORIZATION DONE
|
 | FIG. - 6 Implant migrated labially
|
 | FIG. - 7(a) Impression coping placed
|
 | FIG. - 7(b) Impression
|
The prefabricated angulated abutment (Abutment Selection Kit; Nobel Biocare) was used which was modified by grinding labially to achieve desired cervical profile, angulation, contours, and height to allow for optimal restoration support and esthetics using a three dimensional CAD program (Nobel Biocare, Göteborg, Sweden) (Fig. 8).
The abutment was then digitized using a touch probe scanner (M50; Nobel Biocare AB) and coping was fabricated. It should be noted that abutment and copings was used and to the desire for an esthetic material that closely matched the patient's natural root structure in the area of hard and soft tissue defects, where the abutment would be visible. Healing abutment was removed and custom abutment was secured with 35 N.cm torque. The porcelain fused metal crown was placed, and margin integrity, occlusal relationship, and esthetic was verified (Fig.9). The crown was cemented using resin luting cement (Panavia, Kuraray Medical Co Ltd, Osaka, Japan). The patient recalled regularly for evaluation of long-term success of the restoration for 3 years. She continues to report excellent esthetic, comfort and function, with pleasing smile and excellent outcome.
 | FIG. 8(a) Custom made angulated abutment
|
 | FIG. 8(b) Custom made angulated abutment in mouth
|
 | FIG. 9 Post-operative view
|
Discussion
A technique to resolve severe angulation problems where the UCLA-type abutment was used to fabricate a telescopic coping with the final restoration cemented over the telescopic retainer. This system had the advantage of the hexed index of the UCLA-type abutment to ensure precise, repeatable placement of the abutment. However, the final restoration was cemented, and this may be a disadvantage. Cementation may be undesirable because the restoration cannot be easily retrieved.15
Standard angulated abutments are available from most implant manufacturers, and often these abutments can be used to fabricate an esthetic screw-retained prosthesis. A technique for modifying angled abutments to maximize the esthetic result. Recently a technique that uses a custom-fabricated abutment (IMPAC custom abutment, Vident, Baldwin Park, Calif.) was introduced to correct the angulation of implants. This system incorporates a manually milled screw hole in the custom abutment for the setscrew that retains the final prostheses. There are two major disadvantages to this approach: (1) The technique cannot be applied to single-crown, implant-supported restorations because the system does not contain an anti-rotational component, and (2) It is impossible to transfer the exact position of the initial thread on the implant to the implant analog; therefore the custom abutment may require over or under tightening to ensure precise seating of the overcastting. The system, however, has two significant advantages: (1) It is an inexpensive, uncomplicated technique for creating custom screw holes in virtually any location with the most desirable angulation, and (2) maintenance of a completely retrievable prosthesis is possible.16
A combined technique has been developed that incorporates the advantages of the UCLA-type abutment and the IMPAC custom abutment but eliminates the disadvantages of both systems. Single unit or multiunit implant-supported fixed restorations with favorable esthetics, alignment, and occlusion can be fabricated on mal-aligned implants. The only limitation of this type of abutment is that it looks longer than normal abutment when viewed intra-orally.
Summary
Functional and esthetic restoration of malpositioned implant is possible with the use of angulated abutment and restoration. The use of 3-dimensional CAD technology has contributed to the predictability of such treatment modalities. The ceramic restorative system provided a relatively simple technique for achieving excellent esthetics in the esthetic zone of anterior maxillae.
References
1. Duff RE, Razzoog ME. Management of a partially edentulous patient with malpositioned implants, using all-ceramic abutments and all-ceramic restorations: A clinical report. J Prosthet Dent. 2006 Nov, 96(5):309-12.
2. Stumpel LJ 3rd. The natural tooth pontic; simplified. J Calif Dent Assoc. 2004 Mar, 32(3):257-60.
3. Sierraalta M, Razzoog ME. A maxillary anterior partially edentulous space restored with a one-piece zirconia implant fixed partial denture: a clinical report.J Prosthet Dent. 2009 Jun, 101(6):354-8.
4. Schiroli G. Single-tooth implant restorations in the esthetic zone with Pure Form ceramic crowns: 3 case reports. J Oral Implantol. 2006, 32(4):190-9.
5. Jovanovic SA, Paul SJ, Nishimura RD. Anterior implant-supported reconstructions: a surgical challenge.Pract Periodontics Aesthet Dent. 1999 Jun-Jul, 11(5):551-8
6. Phillips K, Kois JC. Aesthetic peri-implant site development. The restorative connection. Dent Clin North Am. 1998 Jan; 42(1):57-70.
7. Philips K, Kois JC. Aesthetic peri-implant site development. The restorative connection. Dent. Clin north Am. 1998 Jan, 42 (1): 57-70.
8. Touati B, Guez G, Saadoun A. Aesthetic soft tissue integration and optimized emergence profile: Provisionalization and customized impression coping. Pract Periodontics Aesthetic Dent. 1999 Apr, 11(3):305-14; quiz 316.
9. Garber DA, Belser UC. Restoration-driven implant placement with restoration-generated site development. Compend Contin Educ Dent. 1995 Aug, 16(8):796, 798-802, 804.
10. Wohrle PS. Single-tooth replacement in the aesthetic zone with immediate provisionalization: fourteen consecutive case reports. Pract Periodontics Aesthet Dent. 1998 Nov-Dec , 10(9):1107-14.
11. Joseph Y. K. Kan, Goichi Shiotsu, Kitichai Rungcharassaeng, Jaime L. Lozada January. Maintaining and Attenuating Periodontal Tissues for Aesthetic Implant Placement. Journal of Oral Implantology 2000, 26 (1): 35-41.
12. Abrams L. Augmentation of the deformed residual edentulous ridge for fixed prosthesis. Compend Contin Educ Gen Dent.1980 May-Jun, 1(3):205-13.
13. Lazzara RJ. Immediate implant placement into extraction sites: surgical and restorative advantages. Int J Periodontics Restorative Dent. 1989, 9(5):332-43.
14. Schwartz-Arad D, Chaushu G. The ways and wherefores of immediate placement of implants into fresh extraction sites: a literature review. J Periodontol. 1997 Oct , 68(10):915-23.
15. Schmitt SM, Chance DA. A custom titanium implant- retained single-tooth restoration: A clinical report. Int J Oral Maxillofac Implants 1996; 11: 782-786.
16. Lewis S, Avera S, Engleman M, Beumer J. The restoration of improperly inclined osseointegrated implants. Int J Oral Maxillofac Implants 1989, 4:147-52.
|