Introduction:
Odontomas are hamartomas combining mesenchymal and epithelial dental elements. Histologically they are composed of various dental tissues, including enamel, dentin and cementum and in some cases pulpal tissue.They are slow growing, benign, showing non-aggressive behaviour.(1,2,3,4,5) According to the classification of the World Health Organisation (WHO 2005), two types are described; complex and compound odontomes, the latter being twice as common as the former.(6) Eruption of an odontome in the oral cavity is rare. We present a case of a complex odontome in the area of left mandibular molar.
Case Report:
A 28 year old male reported with the complaint of pain in the lower left molar region for the past two months duration. He was apparently healthy and his medical history was non-contributory. (Fig-1) Intra oral examination revealed a yellowish white hard tissue present on the lingual aspect between 37 & 38. The hard tissue resembled a tooth like structure extending subgingivally. The exposed portion measured approximately 5 X 3 mm. The gingiva surrounding the mass appeared apparently healthy. (Fig-2)
 | Figure 1: Patient's photograph
 |
 | Figure 2: Clinical photograph showing the odontome
|
On palpation, it was bony hard in consistency. Based on history & clinical presentation the diagnosis of a supernumerary / retained deciduous tooth was made. Following an informed consent, removal of the tooth like structure was carried out under local anaesthesia. The extracted mass showed no morphological resemblance to any tooth of the normal series. (Fig-3) It measured 7 X 4 mm and a presumptive diagnosis of odontome was considered. The specimen was sent for histopathological examination which showed a homogenous eosinophilic mass suggestive of dentin along with a scalloped dentino-enamel junction and loss of enamel.(Fig-5) Few dilated spaces along with blood capillaries engorged inside are suggestive of pulpal tissue.(Fig-6) Some areas are basophilic suggestive of cementum. These features confirmed the diagnosis of complex odontome.
 | Figure 3: Extracted odontome
|
 | Figure 4: Post extraction site
|
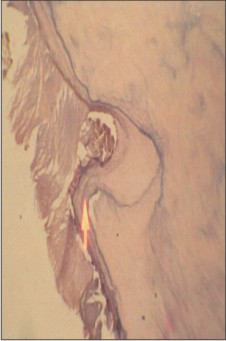 | Figure 5: Photomicrograph (20X magnification) showing dentino enamel junction
|
 | Figure 6: Photomicrograph (40X magnification) showing engorged capillaries
|
Discussion:
Odontomes are one of the most common type of odontogenic tumour and constitute 22% of all odontogenic tumours of the orofacial region.(7,8) They are considered to be hamartomas rather than neoplasms and are composed of tissues native to tooth. Paul Broca (1867) was the first to use the term odontome.(9) In 1914, Gabel et al grouped odontomes based on their developmental origin into epithelial and connective tissue.(10)
In 1946, Thoma and Goldman classified odontomes as follows: (11)
Geminated composite odontomes: Two or more, more-or-less well-developed teeth fused together.
Compound composite odontomes: Made up of more-or-less rudimentary teeth.
Complex composite odontomes: Calcified structure, which bears no great resemblance to the normal anatomical arrangement of dental tissues.
Dilated odontomes: The crown or root part of tooth shows marked enlargement.
Cystic odontomes: An odontome that is normally encapsulated by fibrous connective tissue in a cyst or in the wall of a cyst.
Clinically odontomes are either complex or compound and are classified as :
Intra osseous - they occur within the bone and may erupt into the oral cavity ( erupted odontome)
Extra osseous (peripheral) they occur in the soft tissue covering the tooth bearing areas of the jaws.
Odontomes may present at any age. Although higher predilection is present after 4th decade of life, they are commonly asymptomatic or may present as retention of deciduous teeth, unerupted permanent tooth, pain, cortical expansion and tooth displacement. Occasionally, anaesthesia of the lower lip may be the presenting sign. Complex odontome tends to occur in the posterior region of the jaws, whereas compound odontomes are frequently seen in the anterior maxilla. Odontomes can measure anywhere from a few millimetres to centimetres in greatest dimension.(1)
The largest odontome reported in the medical literature in humans weighed around 0.3kg.(12,13) The first case of an erupted odontome was described by Rummel et al in 1980.(3,14)The etiopathogenesis of odontome formation are many. Odontomes have been associated with trauma during primary dentition, with an inflammatory and infectious processes, hereditary anomalies (Gardener's syndrome, Herman's syndrome), odontoblastic hyperactivity and alteration in the genetic components.(9) Odontomes are also thought to be inherited through a mutant gene during post natal period. During development, the lamina between the tooth germs tends to disintegrate to form clumps of cells. The remnant portion of the lamina may constitute an important factor in the formation of complex or compound odontomes and may present in place of a normal tooth. The mechanism of an odontome erupting appears to be different,due tothe absence of periodontal ligament. Hence the eruptive force varies in both these cases as the former is not linked to the contractility of the fibroblasts. Although there is an absence of anormal tooth morphology, its progressive increase in size may lead to sequestration of the surrounding bone which could result in occlusal movement or eruption. Following eruption, an odontome could cause sufficient bone resorption around it.(1,15)
Bone remodelling of the jaws have also been postulated in the intra oral eruption of odontomas. Different theories have been implicated in the eruption of odontomes both among young and older age group. The resorption of the edentulous part of the alveolar process is thought to play among older people and bone remodelling contributing to the eruption among young individuals.(1,16)
Although odontomes are usually asymptomatic, their eruption into the mouth can give rise to pain, inflammation & infection. Facial asymmetry(1), halitosis(17),
malocclusion (18,19) and recurrent infections have been recorded in association with erupted odontomes. Ferrer et al (20) reported a case of a 22 year old woman with recurrent episodes of infection, malaise, fever and suppuration. In such cases, following broad spectrum antibiotic treatment of the infection, management of odontomes were carried out.
The treatment of choice is surgical removal followed by histopathological study to confirm the diagnosis.
Conclusion:
Odontomes, which are considered to be hamartomatous malformations, are a rare entity when found erupting into the oral cavity. Hence careful clinical evaluation needs to be done to differentiate a retained deciduous tooth or supernumerary tooth from an odontome.
References:
1. Manoj Vengal, Honey Arora, Sujoy Ghosh, Keerthilatha M Pai. Large erupting complex odontoma: A case report. J Can DentAssoc 2007; 73(2): 169-72.
2. Neville BW, Damm DD, Allen CM, Bouquot JF. Odontogenic cysts andtumors. In: Oral and maxillofacial pathology. 2nd ed. Philadelphia (PA):WB Saunders; 2002. p. 631-2.
3. Gabriel Serra-Serra, Leonardo Berini Aytés, Cosme Gay-Escoda. Erupted odontomas: a report of three cases and review of the literature. Med oral Patol Oral Cir Buccal 2009 June; 14(6): E 299-303.
4. Philipsen H, Reichart P, Praetorius F. Mixed odontogenic tumoursand odontomas. Considerations on interrelationship. Reviewof the literature and presentation of 134 new cases of odontomas.Oral Oncol. 1997;32:86-99.
5. Amado Cuesta S, Gargallo Albiol J, Berini Aytés L, Gay EscodaC. Revisión de 61 casos de odontoma. Presentación de un odontomacomplejo erupcionado. Med Oral. 2003;8:366-73.
6. Amailuk P, Grubor D. Erupted compound odontoma: case report of a 15 year old Sudanese boy with a history of traditional dental mutilation. Br Dent J 2008; 204: 11-4.
7. Amado CS, Gargallo AJ, Berini AL, Gay EC. Review of 61 cases of odontoma: Presentation of an erupted complex odontoma. Med Oral 2003; 8: 366-73.
8. Bhaskar SN. Odontogenic tumors of jaws in synopsis of oral pathology. 7th ed. CBS Publishers and Distributors, Delhi 1986. p 292-303.
9. Batra P, Gupta S, Rajan K, Duggal R, Hariprakash. Odontomes - diagnosis and treatment: A 4 case report. J Pierre Fauchard Acad 2003; 19: 73-6.
10. Sunira Chandra, Anjana Bagewadi, Vaishali Keluskar, Kunal Shah. Compound composite odontome erupting into the oral cavity: A rare entity. Contemporary clinical dentistry 2010; 1(2): 123-26.
11. Thoma KM, Goldman HM. Oral pathology. 5thedition. St. Louis: The CV Mosby company; 1960. P 1221-2.
12. Mupparapu M, Singer SR, Rinaggio J. Complex odontoma of unusual sizeinvolving the maxillary sinus: report of a case and review of CT and histopathologicfeatures. Quintessence Int 2004; 35(8):641-5.
13. Wood NK, Goaz PW, Lehnert J. Mixed radiolucent-radiopaque lesions associated with teeth. In: Wood NK, Goaz PW, editors. Differential diagnosisof oral and maxillofacial lesions. Singapore: Harcourt Brace & Company AsiaPte Ltd; 1998. p. 289-314.
14. Rumel A, de Fritas A, Birman E, Tannous L, Chacon P, BorkasS. Erupted complex odontoma. Report of a case. DentomaxillofacRadiol. 1980;9:5-9.
15. Hitchin AD. The aetiology of the calcified composite odontoma. Br Dent J 1971; 130: 475-82.
16. Ten Cate AR, Nanci A. Physiologic tooth movements: eruption and shedding.In: Nanci A, editor. Ten Cate's oral histology: development, structureand function. St. Louis (MO): Mosby; 2003. p. 275-98.
17. Gomel M, Seckin T. An erupted odontoma: A case report. J OralMaxillofac Surg. 1989;47:999-1000.
18. López-Areal L, Silvestre-Donat F, Gil-Lozano J. Compoundodontoma erupting in the mouth: 4 - year follow-up of a clinicalcase. J Oral Pathol Med. 1992;21:285-8
19. Nik-Hussein N, Majid Z. Erupted compound odontoma. AnnDent. 1993;52:9-11.
20. Ferrer M, Silvestre F, Estelles E, Grau D. Infección recurrentede un odontoma complejo tras su apertura a la boca. Med Oral.2001;6:269-75. |