Introduction
Amalgam restorations have been known for their durability and reliability for more than a hundred years. Despite availability of direct tooth coloured restorative materials, amalgam remains a material of choice for posterior restorations. Amalgam is more popular than composite as it is relatively easy to insert, less technique sensitive and has reasonable adequate resistance to fracture. It provides marginal sealing after a period of time in the mouth, has good mechanical properties and is economical for the patient1.
It has a long history of clinical usage with proven longevity2. The dark colour of these restorations presents an aesthetic quandary and has been the chief complaint of many patients. Apart from aesthetics, composite preparation requires less removal of sound tooth structure and improves fracture resistance of teeth. Composites show annual failure rate similar to amalgam2 but the placement of composites is technique sensitive. In case of larger cavities, there is reduced survival rate of the restoration as when compared with smaller cavities3.
Combined amalgam and composite restorations can be a good alternative in some situations. This clinical report will describe a case where an extensive amalgam restoration was covered by a layer of composite for esthetic purpose.
Case Report
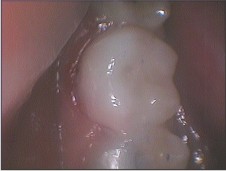
A 20- year-old girl reported to the Department of Conservative Dentistry with the chief complaint of extensive caries in the right mandibular first and second molar (Figure 1) Patient did not report of any history of pain. On examination, it was found that both the teeth had been restored with composite restorations, which were under filled. There was secondary caries around the restorations in both the teeth. First molar was found to be non vital and thus root canal treatment was done and the tooth was finally restored. Vitality testing and radiograph examination revealed a vital pulp without the need of endodontic therapy in second molar. After local anaesthesia, isolation with rubber dam was done. Carious dentin was removed using a round carbide bur under air-water cooling. The cavity configuration was self-retained (Figure 2). A layer of light cure calcium hydroxide (Septocal LC) was applied (Figure 3). Resin modified GIC was used as a base for the final restoration (Figure 4). A high-copper alloy (DPI Alloy) was used to restore the large cavity preparation. Patient was recalled the next day and polishing of the restoration was done (Figure 5). The colour shade was determined and rubber dam was placed. The buccal and occlusal amalgam surface was ground to a depth of 2 mm. Using diamond burs, two small holes were placed in the ground amalgam surface to improve mechanical retention (Figure 6). Resin-modified glass ionomer cement (GIC Gold label light colored universal restorative) was mixed according to the manufacturer's instructions and a thin layer was applied into the retention holes and photo activation was conducted for 40 seconds (Figure 7). The enamel was conditioned with 37% phosphoric acid for 20 seconds followed by washing. Two layers of Adper Single Bond (3M/ESPE) were then applied, which were photo activated for 20 seconds. A layer of masking agent was applied and cured for 40 seconds. The veneer was built with composite (Filter Z250, 3M/ESPE) of the selected tooth shade with two increments of 1 mm each which were polymerized for 40 seconds. Rubber dam was removed; premature contacts were checked and reduced accordingly. The finishing and polishing was completed with finishing burs and disks (Sof-Lex, 3M/ESPE) for the composite (Figure 8).
 | Figure 1: Pre- operative view.
 |
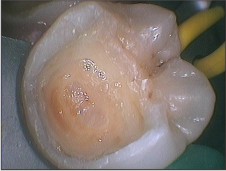 | Figure 2: Cavity preparation after caries removal.
|
 | Figure 3: Light Cure Calcium Hydroxide applied.
|
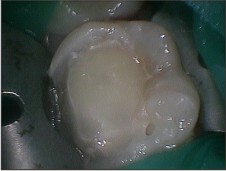
 | Figure 4: Resin modified GIC placed.
|
 | Figure 5: Carved and burnished Amalgam restoration after matrix removal.
|
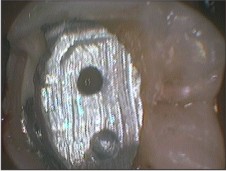 | Figure 6: Amalgam surface reduced and retentive holes prepared in amalgam.
|
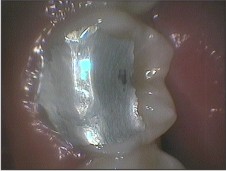
 | Figure 7: Resin modified GIC placed over cut surface on amalgam.
|
 | Figure 8: Composite placed in two increments following enamel etching and application of adhesive system.
|
Discussion
Cast metal restorations are the usual preferred restoration for teeth requiring extensive coronal reconstruction4. In cases where patient demands for aesthetics, desires to save the remaining sound tooth structure and expresses their inability to afford indirect restoration; it leaves the dentist with no option other than direct composite restoration. Accurate marginal adaptation and polymerisation shrinkage are the concerns with composite restorations in extensively decayed teeth with vital pulp.
The case reported shows a technique that combines the excellent mechanical properties of amalgam with aesthetics of composite. In order to provide some mechanical retention between amalgam and composite; amalgam was ground with a diamond bur and small holes were prepared. These holes improve the resistance to displacement of composite caused by occlusal forces5.
Resin modified GIC was added as a layer to bond amalgam with composite for three reasons.
1) RMGIC has bonding capacity to both materials6.
2) The interface will be filled with a compatible material thus the composite, amalgam and interface will be properly sealed.
3) The gray colour of amalgam is masked properly7.
Masking agent was used as a first layer of composite to enhance aesthetics. Acid etching was done only on the enamel surface since some studies have found reduction in bonding resistance between materials thus increasing micro leakage8-9.
The use of resin composite material as a material to restore occlusion is controversial and data supporting it is scarce. On evaluating posterior vertical bite reconstruction using direct posterior composites, Schmidlen PR, Filli T, Imfeld C, Tepper S, Attin T10 observed that occlusion of extensively worn teeth can be restored using direct posterior composites. Present day resin bonded composites exhibit mechanical and physical properties superior to those of their predecessors. Wear of direct resin composites is exhibited to be around 10-15µ per year while amalgam wears about 10µ per year more than enamel. Thus the wear rate or both the restorations is similar.
Conclusions
Composite veneering represents a good alternative for the aesthetical improvement of extensive amalgam restorations as the dark color of these restorations is masked by the tooth color appearance of composite. The patient is thus satisfied with the final restoration.
References:
1. Gil FJ, Espias A, Sanchez LA, Planell JA. Comparison of the abrasive wear resistance between amalgams, hybrid composite materials and different dental cements. Int Dent J. 1999; 49(6):337-42.
2. Manhart J, Chen H, Hamm G, Hickel R. Buonocore Memorial Lecture. Review of the clinical survival of direct and indirect restoration in posterior teeth of the permanent dentition. Oper Dent. 2004; 29(5):481-508.
3. da Rosa Rodolpho PA, Cenci MS, Donassollo TA, Loguercio AD, Demarco FF. A clinical evaluation of posterior composite restorations: 17 year findings. J Dent 2006; 34(7):427-35.
4. Barkmeier WW, Cooley RL. Amalgam restoration with a composite resin window. Quintessence Int Dent Dig.1979 April; 4:31-4.
5. Burgess JO, Alvarez A, Sumitt JB. Fracture resistance of complex amalgam restorations.Oper Dent.1997; 22(3):128-32.
6. Cenci MS, Piva E, Potrich F, Formolo E, Demarco FF, Powers JM. Microleakage in bonded amalgam restorations using different adhesive materials. Braz Dent J. 2004; 15(1): 13-8.
7. Plasmans PJ, Reuters EA. Esthetic veneering of amalgam restorations with composite resin window- combining the best of both worlds? Oper Dent.1993; 18(2):66-71.
8. Hadavi F, Hey JH, Ambrose ER. Shear bond strength of composite resin to amalgam: an experiment in vitro using different bonding systems. Oper Dent. 1991; 16(1):2-5.
9. Hadavi F, Hey JH, Ambrose ER. Assessing microleakage at the junction between amalgam and composite resin: a new method in vitro. Oper Dent. 1991; 16(1):6-12.
10. Scmidlin PR, Filli T, Imfeld C, Tepper S, Attin T. Three-year evaluation of posterior vertical bite reconstruction using direct resin composite-- a case series. Oper Dent. 2009;34(1):102-8. |