Introduction
Loss of tooth in the esthetic zone of the anterior region can be due to trauma, periodontal disease or endodontic failure. Replacement can be provisional, semi-provisional or permanent in nature. Depending on multiple factors, a treatment module is decided upon by the dentist and patient. The start of the definitive treatment depends on many factors and thus may require short to long temporization times. Final restorations can vary between removable prosthesis, tooth-supported prosthesis or implant-supported prosthesis. Irrespective of the final treatment, the first line of treatment would be to provisionally restore the patient's aesthetic appearance while functionally stabilizing the compromised arch.
Case Report
A 34 year old female reported to the Department of Periodontology and Implantology, Sardar patel post graduate institute of dental and medical sciences, Lucknow with a chief complaint of missing tooth no. 31
On examination, the patient was diagnosed to have chronic generalized periodontitis with grade II mobility in 41, 42, and 32. Preoperative photographs and radiographs were taken (Fig.1 and 2). On radiographic examination, the periodontal health of the 41, 42 and 32 were not favourable for fixed prosthesis. The patient's periodontal health was assessed to be poor and a full mouth scaling and root planing was performed and the patient was recalled after a week (Fig 3). The patient showed a remarkable improvement in her periodontal health.
 | Fig 1. Pre-Op Frontal View Showing Missing 31
 |
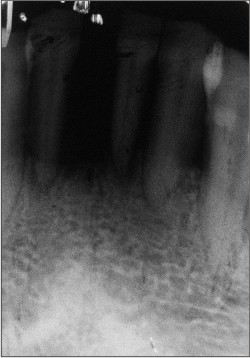 | Fig 2. Pre-Op Radiograph Showing The Amount Of Bone Loss
|
 | Fig 3. Frontal View After Phase I Therapy
|
Technique
1. After the root canal therapy of 41, 42 and 32 (Fig 4), the selected abutment teeth (32, 33, 41, 42 and 43) were prepared with a horizontal lingual groove to accommodate a stainless steel 24 gauge wire (Fig 5). The groove was approximately 1.5 to 2 mm deep and 0.5mm wide.
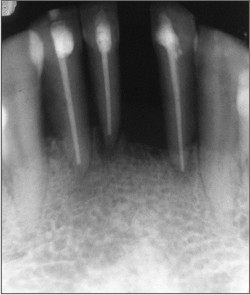 | Fig 4. Post Op Radiograph After Completion Of Endodontic Treatment
|
 | Fig 5. Grooves Prepared On The Lingual Surface For Placement Of Splint
|
2. A rubber based diagnostic impressions were made and cast prepared. The artificial tooth pontic was measured with a periodontal probe to the length needed. The acrylic tooth was shaped with a flame-shaped finishing bur.
3. The positional relation and the length of the prepared pontic were checked using the diagnostic cast. The occlusion was carefully evaluated and adjusted to ensure proper contact relations with adjacent teeth (Fig 6).
 | Fig 6. Acrylic Tooth Selected And Mock Preparation Done
|
4. The length of the 24 gauge stainless steel wire was determined by placing a piece of dental floss from the distal surface of right canine (43) to the distal of the left canine (33), and a piece of the wire was cut to this length.
5. The pontic and the abutment teeth were etched with 37% ortho phosphoric acid.
6. The artificial tooth pontic and abutment was prepared for bonding by first wetting it with a bonding agent (Single Bond; 3M ESPE) and was light-cured for 10 seconds.
7. The wire was placed in the prepared groove of the lingual surface of artificial tooth pontic. A layer of flowable composite resin was injected into the groove and was light-cured for 40 seconds (Fig 7).
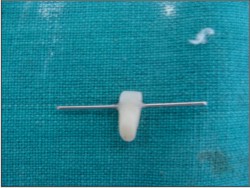 | Fig 7. Splint Stablized On The Acrylic Tooth
|
8. The wire bonded with the pontic, was then placed into the prepared lingual grooves of the abutment teeth. A layer of composite resin was placed on top to secure it in place. The restoration was light-cured for 40 seconds
9. Occlusal interferences were evaluated. The lingual aspect of the provisional restoration was polished with an abrasive impregnated rubber finishing system.
10. The pontic was kept in contact with the gingival tissue to simulate a correct emergence profile and gingival contour. The opposing teeth were kept out of contact with the pontic at rest and in function (Fig 8 and 9).
 | Fig 8. Post-Op Frontal View After Stabilization Of Acrylic Tooth In The Edentulous Space
|
 | Fig 9. Post-Op Lingual View
|
Discussion:
A resin-bonded anterior fixed partial denture (RBFPD) is a well established option for the replacement of missing teeth and the success rate is reported to be 76% after 5 years and 60% after 10 year1. Replacement of missing teeth with RBFPD is a non-invasive restorative treatment. This concept has reduced the risk of critical loss of tooth structure and provides the maintenance of optimal strength, form and esthetic2. Conventional materials, namely metal alloy and ceramics, are used in prosthetic dentistry because of their rigidity.3 The rigidity of the material makes it impossible to use enamel surfaces with undercuts as a bonding surface. For this reason, the conventional type of RBFPD is made with relatively small bonding surface area4 and it saves time too.
Alone, composite resin is a brittle material, incapable of withstanding prolonged occlusal forces, especially as an unsupported pontic.5. The conservative metal-reinforced composite resin pontic will provide, for a relatively long time, functional and cosmetic space maintenance in such individuals.6
Summary & Conclusions:
Resin-bonded fixed partial dentures (FPDs) have been used for dental treatment for many years. Although early resin-bonded FPDs were associated with a high frequency of premature failure, better understanding of preparation design and improved bonding techniques have led to significant improvements in their long-term survival7. The primary reason for prescribing a wire reinforced composite resin-based provisional FPD, was the desire for better stability of the pontic along with the mobile adjacent teeth in the mandibular anterior region and to meet the patient's expectations.
References:
1. Sadeghi M. MS: Bond strength of glass fiber reinforced composite and base metal frameworks used in resin-bonded fixed partial dentures. Beheshti Univ Dent J 2005; 22(Special Issue): 95-99
2. Bouillaguet S, Schutt A, Marin I, Etechami L, Di Salvo G, Krejci I: Replacement of missing teeth with fiber reinforced composite FPDs: clinical protocol. Pract Procde Aesthet Dent 2003; 15: 195-202
3. Vallittu PK. Case report: A glass fibre reinforced composite resib bonded fixed partial denture. Eur J Prosthodont Rest Dent 2001; 9: 35-9
4. Nicholson JW: Adhesive dental materials.A review. Int J Adhesion 1998; 18: 229-36.
5. Ian E. Shuman. Replacement of a tooth with a fiber-reinforced direct bonded restoration, General Dentistry May - June 2000
6. Dan Nathanson and Kambiz Moin. Metal-reinforced anterior tooth replacement using acid-etch-composite resin technique. THE JOURNAL OF PROSTHETIC DENTISTRY APRIL 1980 VOLUME 43 NUMBER 4
7. el-Mowafy O, Rubo MH. Resin-bonded fixed partial dentures-a literature review with presentation of a novel approach. Int J Prosthodont 2000;13: 460-7. |