Introduction
The size and shape of the arches have considerable implications in orthodontic diagnosis and treatment planning, affecting the space available, dental aesthetics, and stability of the dentition1-2. The use of preformed arch wires is widespread in orthodontics. Identification of the dental arch form of the orthodontic patient is an important parameter in achieving a stable, functional, and esthetic dentition. Failure to customize preformed arch wires with the patient's arch form might increase the probability of relapse and lead to an unnatural smile3.
Technological advances in materials, with the use of new arch wires and appliances, have certainly enabled to obtain achievement of rapid results during phase of alignment and leveling between arches4. Improperly formed arch wires create and contribute too many post treatment problems. Unplanned contraction or expansion, especially in the cuspid or molar region, produces instability. Correct cuspid or molar width should be determined and decided upon as an integral part of the diagnostic procedure and once these widths have been established, they should be maintained throughout treatment. This will prevent unnecessary movement of the teeth which is undesirable and could cause tissue damage. Maintaining symmetry is very important in forming archwires. Asymmetrical wires leave the anterior or buccal segments out of harmony and make midline deflections difficult to correct5.
The mandibular dental arch is considered as major reference element of diagnosis and therapy in dentofacial orthopedics6. According to Braun and Legan7, the stability of the form and dimensions of mandibular dental arch is a factor of stability of therapeutic results. The process of individualizing arch forms from the original mandibular arch has become popular8-9. Various studies have used normal, untreated study casts for determining arch form mathematically or for characterizing arch form through various measurements, with incisal edges, cusp tips and molars cusps as landmarks10.
Boone has suggested that the individuality of a patient's arch form and dimensions must be recognized and respected if a successful treatment outcome is to be achieved11. Many believe that arch form and size are unique for each individual and are principally controlled by the form of the basal bones12. Arch form and size should be recognized as part of a morphologic human pattern13-15. With these considerations in mind, an investigation is undertaken to evaluate the mandibular dental arch form and prefabricated stainless steel arch forms.
Arch wires are vital and active part of orthodontic appliance. They store and deliver power through brackets and bands, to teeth and surrounding tissues5. Today in the era of competition and limited time availability among people prefabricated arch wires has become popular among orthodontist to save time and also not compromising treatment results. Commercially two forms of Stainless steel arch forms (Euro form, Standard/ Trueform/ Natural) are marketed commonly by most Companies (Dentsply, Modern, Orthotech, Rabbit force).
So the primary objective of this study is to do intercompany comparisons of 4 companies (Dentsply, Modern, Orthotech, Rabbit force) for goodness of fit of 0.016” stainless steel Standard and Euroform arch form at three transverse dimensions in Himachali ethnic population and second objective is to compare whether there is difference in use of Standard or Euroform for different malocclusion groups.
Material And Method
This study was conducted in the Department of Orthodontics, Himachal Dental College, Sundernagar. Sample consisted of 75 pretreated mandibular casts of patient of age group 12 to 20 years of Himachali ethnic origin was taken.
They were divided into 3 groups-
Group 1- Angles Class I (n - 25)
Group 2- Angles Class II Div I (n - 25)
Group 3- Angles ClassII Div 2 ( n - 25)
All the casts met the following inclusion criteria-
(1) Angle's dental Class I, II div 1 and III malocclusions.
(2) Permanent dentition with normal tooth size and shape
(3) 3-mm or less arch length discrepancy.
(4) Clinically acceptable symmetry of mandibular dental arch.
The occlusal photographs of mandibular cast were taken with a digital camera Nikon D-40 macrolens (Nikon corporation, Tokyo, Japan). Camera was mounted on tripod stand and photographs were taken according to the method described by Naif Almasoud and David Bearn16. According to this method photographs were taken parallel to long axis of Incisors teeth (Perpendicular position 90) considering the ideal projection. This ideal projection shows the labial and lingual surfaces of the anterior teeth(Fig 1a)
 | Fig 1A
 |
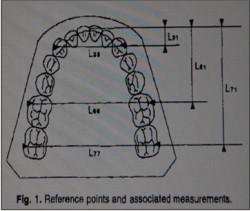
The image was then imported into the Image J software. Saggital and transverse measurements of mandibular dental arches were done from the casts using this software. They were taken from the following reproducible reference points: the midincisal edge (Buccal Side), the canine cusp tips, mesiobuccal cusp tips of first molars and the distobuccal cusp tips of second molar. These points constitute the landmarks of mandibular dental arch form. They define the breaking points of the arch and limit sectors on which different muscle groups have an action. The precision gained by the use of other points would be minimal because of the strong correlations observed between the different measurements taken from these points. Dimensions of the dental arches were determined according to the three saggital and three transverse measurements 9 (Fig 1b)
 | Fig - 1B
|
Arch breadth was evaluated from4(Fig 1b)
1) Intercanine width - Canine cusp tips(L33)
2) Mean Intermolar width - Between mesiobuccal cusp of first molars (L66)
3) Posterior Intermolar width - Between distobuccal cusp of 2nd molar (L77)
Arch length was evaluated from4 (Fig 1b)
1) Canine depth - Arrow of the anterior curve(L31)
2) Mean arch length - From the incisal edge to the line joining the mesiobuccal Canines of first molars(L61)
3) Total Length - Incisal edge to line joining the disto buccal cusp of the second molars. (L 71)
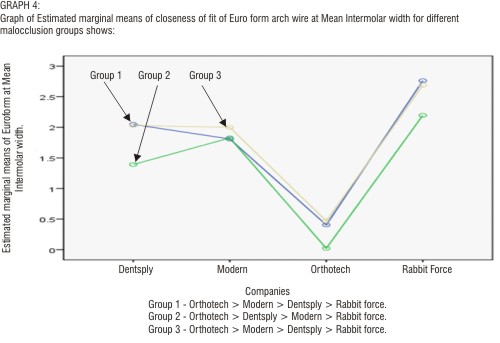
These measurements were used to prepare graphs (Fig 2). Graphs were plotted with these six measurements. On graphs prefabricated arch forms 0.016” Stainless steel were superimposed and goodness of fit of Standard and Euroform of four companies (Dentsply, Modern, Orthotech, Rabbit force) were measured at Intercanine width, Mean Intermolar width, Posterior Intermolar width on plotted graphs for different malocclusion groups studied.
 | Fig - 2
|
Result
Discussion
Since the time of Edward Angle, orthodontists have tried to determine the ideal arch form or “true line of occlusion”. Many different solutions to this problem have been proposed, but few have stood the test of time1. As the use of super elastic and preformed stainless steel arch wires becomes common among orthodontists aiming to achieve optimal alignment of dental arches, the identification of the patient's dental arch form is an important parameter in achieving a stable, functional, and esthetic dentition17,20
The results of this study tend to support previous findings suggesting that there is no single, universal, ideal arch form applicable to all cases18. Biologic variability appears to be so great that even in a sample of untreated normal cases, no predominant arch form could be identified1. So the primary objective of this study was to do intercompany comparison to know whether there is any company differences in dimensions of prefabricated arch forms i. e. (Standard / Euroform) for different malocclusion groups and secondary objective was to compare Standard form with Euroform. The difference in dimensions of prefabricated arch forms i.e. (Standard / Euroform) of different companies for different malocclusion groups are as follows:
 |
|
 |
|
 |
|
 |
|
 |
|
 |
|
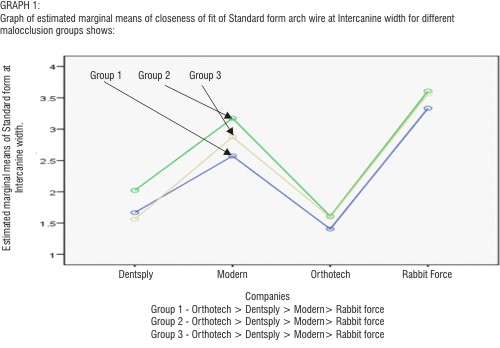
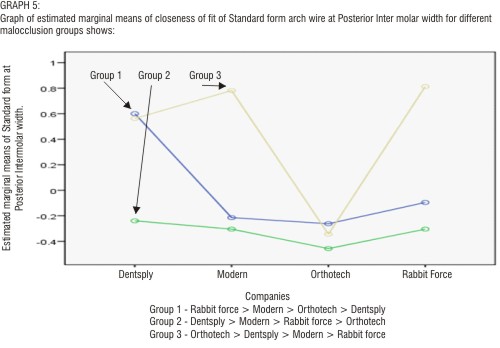
1. For Standard Arch form (Graph 1,3&5) result showed that closeness of fit sequence is Orthotech > Dentsply > Modern > Rabbit force at Intercanine width and at Mean Intermolar width showing Standard arch form is narrow in anterior and molar region for Orthotech and wider in anterior and molar region for Rabbit force in all malocclusion groups. This is in accordance with the study conducted by Felton et al1 who reported that there was a little difference between arch forms of Class 1 and Class II malocclusion groups. Our results were also supported by the study conducted by Nojima et al19 who stated that Class I arches were deeper than the Class II arches with little difference in arch width between the two ethnic groups.
2. The closeness of fit sequence at Posterior Intermolar width was not consistent for all malocclusion groups for Standard form.
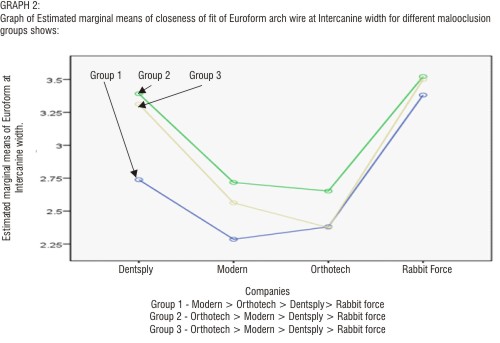
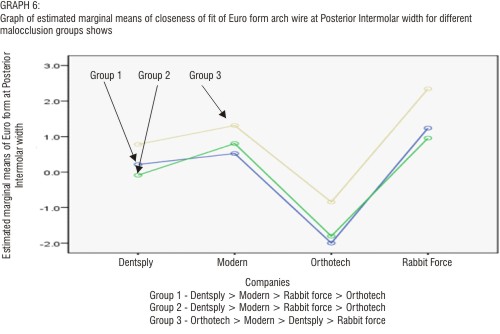
3. For Euroform result showed that closeness of fit sequence does not match at Intercanine width, Mean Intermolar width and Posterior Intermolar width for all three groups.
Our result (Table 1) showed that there was no differences between Standard and Euroform for Group 1, Group 2 and Group 3 for Rabbit force Company as significant values come for all. For Dentsply significant values came for all except in Group 1 at 1st Mean Inter molar width. For Modern result are significant for all except in Group 2 at Mean Intermolar width. For Orthotech Results are significant for all except in Group 1 at Mean and Posterior Inter molar width in Group 2 at Mean Intermolar width and for Group 3 at Mean Intermolar width. So these values are consistent with our result as Orthotech had best fit for Standard forms for all three groups in Intercanine and Mean Intermolar width and Rabbit force has poorest fit. So the results of our study is in favour of the study conducted by Yossi et al20 analysis of Israeli sample indicated that, as malocclusion shifts from Class III through Class I to Class II , the weight of arch form tends to shift from square and ovoid to ovoid and tapered. This clearly indicates that interarch relationship affect mandibular arch forms. This is also supported by Braun et al21 stated in their report on differences in arch dimensions between Angles classes that the Class II mandibular arches exhibited generalized reduced arch width and depth compared with the Class I arches. As studies are lacking in this field, so further studies are awaited to come to a final conclusion whether there is any intercompany variation in closeness of fit of arch forms for different malocclusion groups.
 | Table 1 shows Paired correlation coefficient between Standard form and Euroform of different companies when superimposed on graphs at Intercanine width, Mean Intermolar width, Posterior Intermolar width. Result shown for different company's are-
|
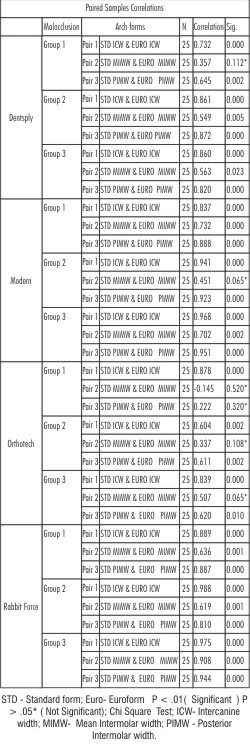 | TABLE 1 Shows Paired Samples Correlations coefficient test between Standard and Euroform of different companies for different malocclusion groups
|
Conclusion
The following conclusions were drawn from this study :
1. For Standard Arch form (Graph 1, 3 & 5) result showed that closeness of fit sequence is Orthotech > Dentsply > Modern >Rabbit force at Intercanine width and at Mean Intermolar in all malocclusion groups , at Posterior Intermolar width sequence is not consistent for all malocclusion groups.
2. For Euroform result showed that closeness of fit sequence does not match at Intercanine width, Mean Intermolar width and Posterior Intermolar width for all three groups.
So we conclude that no company can be said to have best fit as results vary for both Standard and Euroform at three transverse dimensions for all groups.
Bibliography
1. Felton JM, Sinclair PM, Jones DL, Alexander RG. A computerized analysis of the shape and stability of mandibular arch form. Am J Orthod Dentofacial Orthop 1987; 92: 478-83.
2. Strang R. Factors of influence in producing a stable result in the treatment of malocclusion. Am J Orthod Oral Surg 1946; 32:313-32.
3. Ricketts RM. A detailed consideration of the line of occlusion. Angle Orthod 1978 ; 48:274-82.)
4. Raberin M, Laumon B, Martin J, Brunner F. Dimensions and form of dental arches in subjects with normal occlusions. Am J Orthod Dentofac Orthop. 1993; 104: 67-72Boone Gig
5. Boone G. Arch wire designed for individual patients. Angle orthod 1963 33: 178-85.
6. Little R.M, Wallen TR, Riedel R.A- Stability and relapse of mandibular anterior alignment. First premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod 1981; 80 : 349-65
7. Braun S et al. An Evaluation of the shape of some popular nickel titanium preformed arch wires. Am J Orthod Dentofacial Orthop 1999;116: 1-12)
8. Robertt JH. Segment concept in arch pattern design. Am J Orthod 1980; 77: 355- 67.
9. Andrews LF. The six keys to occlusion. Am J Orthod 1972; 62: 296- 309.
10. Merz ML, Isaacson RJ, Germane N, Rubenstein LK. Tooth diameters and arch perimeters in a black and a white population. Am J Orthod Dentofacial Orthop 1991; 100:53-8.
11. Wehrbein H, Fuhrmann RAW, Diedrich PR. Periodontal conditions after facial root tipping and palatal root torque of incisors. Am J Orthod Dentofacial Orthop 1994; 106 :455-62
12. Braun S, Bluestein M. A new concept: impulse in orthodontics. Am J Orthod Dentofacial Orthop 1997; 111:437-40.
13. Brader AC. Dental arch form related with intraoral forces. Am J Orthod 1972; 61:541-60.
14. Weinstein S. Minimal forces in tooth movement. Am J Orthod 1967; 53:881-903.
15. White LW. Individualized ideal arches. J Clin Orthod 1978; 11: 779-87.
16. Almasouda N and Bearn D. Little's irregularity index: Photographic Assessment vs study model assessment Am J Orthod Dentofacia Orthop 2010; 138:787 -94.
17. Kook YA, Nojima K, Moon HB, McLaughlin RP, Sinclair PM. Comparison of arch form between Korean and North American white populations. Am J Orthod Dentofacial Orthop 2004; 126: 680- 6 .
18. White LW. Individual ideal arches. J Clin Orthod 1978; 12: 779-87.
19. Nojima K, McLaughlin RP, Isshiki Y, Sinclair PM. A comparative study of Caucasian and Japanese mandibular clinical arch forms. Angle Orthod2001; 71:195- 200.
20. Gafni Y et al. Comparison of arch forms between Israeli and North American white populations Am J Orthod Dentofacial Orthop 2011;139: 339-44).
21. Braun S, Hnat WP, Fender DE, Legan HL. The form of the human dental arch. Angle Orthod 1998; 68: 29-36. |