Key Messages
Special attention should focus on the facts that injections, solutions and equipments are frequently purchased outside the healthcare system and injections are dispensed by unqualified personnel in pharmacies or marketplaces. It is worth reiterating that the majority people infected with hepatitis C are unaware of their infection, so sterilization, disinfection and general hygiene is important.
Introduction:
Before testing for the hepatitis C virus was developed in 1989, it became apparent that some people receiving blood transfusions and blood products were contracting hepatitis, despite the fact that blood and blood products were screened for hepatitis B (HBV) and Hepatitis A (HAV). The majority of these cases, known as non A- non B - Hepatitis or post transfusion hepatitis have since been identified as Hepatitis C (HCV). The impact of this infection is just emerging in India. India's blood banking system has serious shortcoming. Another serious malaise in our health system is the sense of improperly sterilized needles. Both these factors are potential source for the spread of Hepatitis C in India.
Prevalence
The World Health Organization estimates that 170 million are infected with Hepatitis C world wide and 3-4 million persons newly infected each year. Although HCV is endemic worldwide, there is a large degree of geographical variability in its distribution. Countries with the highest reported prevalence rates are located in Africa and Asia; areas with lower prevalence include the industrialized nations in North America, Northern and Western Europe and Australia.
There is wide range of prevalence estimates among developing countries and generally less data available to validate assumptions about the burden of the disease than in the developed world.
China, whose citizens' account for 1/5th of the world's population has a reported seroprevalence of 3.2%. In India which holds an additional 1/5th of the world's population, one community based survey reported an overall rate of 0.97%, Indonesia rate is 2.1% but is based on sero surveys of voluntary blood donors, In Pakistan the most reported range is between 2.4% and 6.5%. Egypt, with an estimated population of 73 million has the highest reported seroprevalence rate of 22 %.1
Aim
The purpose of this paper is to raise awareness regarding the burden of the disease related to viral hepatitis and the need for urgent action to prevent hepatitis C virus. The cost to treat patients with HCV infection far outweighs the cost of implementing prevention programs.
A comprehensive strategy is urgently needed to prevent transmission of these blood borne pathogens. We should educate everybody about the risk of blood borne pathogen transmission in the health care setting. Urgent efforts are needed to ensure patient safety, infection safety, safe dental care and quality assurance in health care.
In providing effective dental care to people infected with the hepatitis C virus, the first step is an understanding of the virus and the potential health and dental health problems associated with hepatitis C infection and issues of infection control and prevention of disease transmission.
The Virus
Hepatitis C is a RNA virus belonging to the flavivirus family and genus hepacivirus. Genetically distinct viral groups have evolved with nine different genotypes of hepatitis C identified and approximately 40 different genotypes. 2
Clinical outcomes in HCV infection: - Initial clinical signs of infection with HCV are often mild. Acute infection is often subclinical and because of this many cases go unrecognized. When symptoms do occur they include malaise, nausea, upper right abdominal pain and jaundice.
Following primary infection, 15-20% of patients clear the virus within 2-6 months. The remainder 80- 85% of cases will develop chronic HCV infection; of these 20% of patients with chronic HCV will not develop any significant liver damage. The remaining chronic infected patients can have a variety of problems relating to long term infection with HCV. For example 20-25% of patients will develop cirrhosis.3 It is thought that the development of cirrhosis is compounded by other factors such as age of the patient (>50years), gender (M>F) and high alcohol consumption. Long term consequences of cirrhosis are liver failure or liver cancer.
In addition to the specific liver pathology, extra hepatic manifestations of HCV infections include glomerulonephritis, cryoglogulinaemia, polyarteritis nodosa, vasculitis, peripheral neuropathy, thyroid dysfunction, non- Hodgkin's lymphoma, thrombocyopenia, lichen planus and sjogren's syndrome. The three latter conditions are of particular significance in a dental setting and the patients with HCV infection require a thorough investigation (including complete blood examination and liver function tests) if invasive procedures are planned. 3
Transmission
Hepatitis C is mainly transmitted via blood to blood contact. The most important routes of transmission are:-
1. Blood transfusion is an effective mode of transmission of hepatitis C infection as it allows a large quantum of infective virions into susceptible patient. In developed countries numerous corrective measures have reduced the spread of infection through this route. In India, mandatory screening for HCV was introduced as late as 2002.
2. IV drug abuse: - Transmission of hepatitis C occurs with IV and percutaneous drug abuse. This is a significant problem in northeast India and Definitely in the rest of country as well. In the study the prevalence of HCV was alarming 92% among 77 IV drug users from Manipur. 4
3. Dialysis and renal transplant: - patients on haemodialysis are at increased risk for hepatitis C as a result of cross contamination from dialysis circuits.5
4. Health care workers are at a higher risk as they come in contact with potentially infected patients. Dentists were found to have significantly high prevalence of HCV with an estimate of 5.4% in a study reported from Rajasthan.5 Transmission by saliva alone is remote possibility unless the saliva is contaminated with blood. However one study supports the concept that gingival crevicular fluid may be a significant source of HCV in saliva. 6
Other less common routes of infection are
1. Mother to baby contact before or during birth. HCV mother to child transmission in HIV infected women is high.
2. Sharing razors or toothbrushes which have been contaminated with blood.
3. The risk of transmitting hepatitis C via sexual contact is considered extremely low. It may occur if there is blood to blood contact during sex.
Punjab leads in Hepatitis C Cases:
According to a report the state has maximum number of hepatitis C cases. Out of 200 million suffering from hepatitis C, 25 million are Indians and the state shares a percentage of almost 5-7% of the sick. What is more striking is that whereas one out of every 12 persons is suffering from hepatitis virus in world, the ratio is one out of every 16 people in Punjab.
According to report in Times of India, 30 September, 2009 at least 142 cases of Hepatitis B and Hepatitis C have been seen in the Baghapurana and Nihalsingh wala subdivisions of Moga sub district. This outbreak is due to use of inadequately sterilized needles and syringes by unqualified medical practioners. Patients are given injections instead of medicines so as to give fast relief is the reason for HCV to become active in this area. Despite having knowledge about parenteral route of transmission of HCV infection, a sizeable proportion of family physicians in the Punjab state continue to reuse needles and syringes.7 Prevalence of active hepatitis C virus infection in apparently healthy inhabitants of district Faridkot, was surveyed during Dec 2009 to Dec 2010. The results showed that 15% of the people of districts Faridkot are actively infected with HCV. It was also concluded that the prevalence of active HCV infection was high (73%) in males as compared to the females (26%). 8
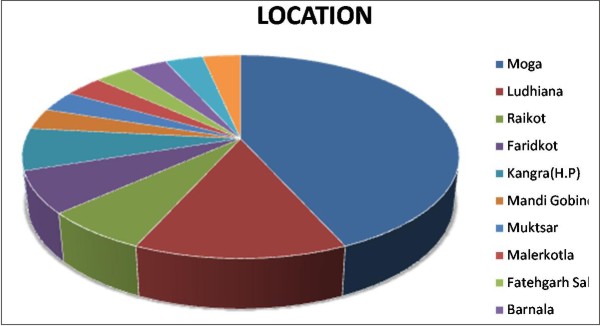
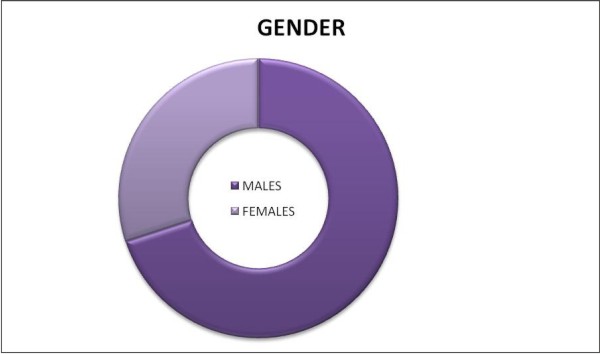
In our Dental Department we have received 30 cases of Hepatitis C in 3 month duration. Out of these 30 cases 13 are from villages of Moga district, one from Mandi Gobindgarh, one from Muktsar, two from Raikot, one from Malerkotla, two from Faridkot, one from village of Fatehgarh sahib,four from Ludhiana district, one from Barnala, two from Kangra(H.P.), one from Fatehabad (Harayana), one from Mansa . Out of these 21 are adult male patients and nine are females. One patient from village charanwal of Barnala district and one from village Walipur of Ludhiana district told that their whole family members and many others families of the same village were going to a particular physician and all of them are found to be HCV positive. This is really an alarming situation.
Probable root cause of infection in 17 out of 30 patients were getting injections for various ailments from quacks. Two patients were chronic alcoholic and drug addicts, rest of the patients were unaware of the cause of infection. Most patients were having non-specific symptoms such as body aches, improper digestion, loss of appetite, weakness and were diagnosed during routine examination or during admission in hospital for any type of surgery.
Chief Dental Complaints
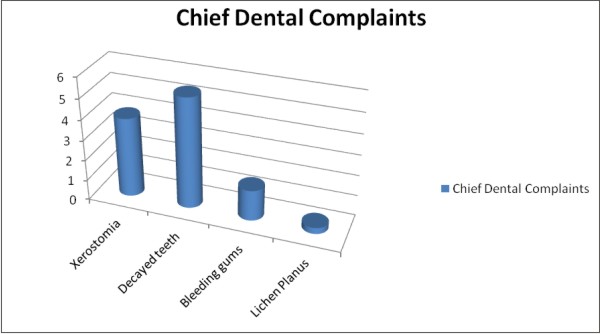
1. Xerostomia - complaints of dry mouth was found in 13 out of 30 patients. Xerostomia can be attributed to variety of causes including medications such as antidepressants and methadone, Sjogren's syndrome associated with HCV can also cause dry mouth.
2. Decayed teeth - Multiple decayed teeth were found in 18 out of 30 patients. The main cause of tooth decay is xerostomia and poor dental health. In two patients, large periapical abscess were found in relation to decayed teeth (Fig 1, Fig 2). This can be due to decreased immunity of these patients. Antiviral drugs such as interferon, ribavirin and corticosteroids may lower resistance to infection. Coates E.A et al also found increased incidence of tooth decay in Hepatitis C patients.9
3. Bleeding gums - Bleeding gums were found in 5 out of 30 patients. This can be due to poor oral hygiene and thrombocytopenia. In patients with cirrhosis, there is likelihood of prolonged bleeding following dental procedures caused by a lack of coagulation factors and thrombocytopenia. Consequently, any invasive dental treatment (extractions, surgery and extensive periodontal treatment) should be undertaken after consultation with appropriate medical specialist.
In one patient periodontal abscess was found in both upper lateral incisors were seen which did not respond to drugs and periodontal therapy. (Fig 3)
4. Lichen Planus - The association of LP with hepatitis C (HCV) has been widely reported in the literature. However, there are wide geographical variations in the reported prevalence of HCV infection in the patients with Lichen Planus. 10 In our study of 30 patients we found only one case of lichen planus with HCV.
 | Fig 1- Periapical radiolucency in relation to 45.46 and multiple decayed and missing teeth.
 |
 | Fig 2- periapical radiolucency in relation to 16
|
 | Fig 3- periodontal abscess in relation to 12. 22.
|
Prevention and Infection Control
Hepatitis C is a notifiable disease. The risk of sexual transmission is extremely low. People with Hepatitis C should be advised not to share household items which may carry traces of blood such as toothbrushes, razors, shavers, dental floss or barber's hair cutting equipment, and not to reuse injecting needles. The virus is not transmitted via hugging, kissing or touching.
Standard Precautions
Standard Precautions are recommended for the care and treatment of all patients and in handling of-
1. Blood
2. All other body fluids, secretions and extractions (excluding sweat), regardless of whether they contain visible blood
3. Non intact skin
4. Mucous membrane
Standard Precautions include
1. Aseptic technique
2. Hand washing
3. Use of appropriate protective equipment gloves, gowns, plastic aprons, masks/ face shields and eye protection
4. Appropriate reprocessing of instruments and equipment
5. Implementing environmental controls
Needle stick injury and blood spills
At the time of needle stick injury or other exposure
Skin - wash with soap and water
Mouth, nose, eyes - rinse well with water or saline. Report the incident and follow your local workplace Occupational Exposure Protocol
Conclusion
Hepatitis C is an emerging infection in India whose long term implications will be felt in the decades to come. It is a pathogen that is already responsible for significant proportion of liver disease in various regions of India. Stringent blood banking laws needs to be introduced and sterilization and reuse of needles discouraged. All this is not possible without increased public awareness of the magnitude and implications of this chronic infection and its mode of spread.
Not all people with hepatitis C know that they have the virus. Unlike HBV, where an effective vaccine exists, no such vaccine is available to protect against HCV infection. Patients are not obliged to inform dentists that they have contracted the virus because adherence to the Universal Precaution System, where every dentist patient encounter is considered to have the potential for cross infection, should minimize the risk of new cases of hepatitis C occurring.
References:
1. Shepard CW, Finelli L and Alter MJ. Global epidemiology of Hepatitis C Virus infection; Lancet Infect. Dis. 2005; 5:558-567.
2. Dental Health and Hepatitis C. www.ashm.org.an/publication
3. Dr.S R Prabhu,Dr.Bhasker Rao, Dr. Anil Kohli; HIV and AIDS in dental practice 2007.
4. Saha M.K, Chakrabarti S, Panda, S, Naik TN, Manna B, Chatterjee A, Detels R and Bhattacharya S.K. Prevelance of HCV and HBV infection amongst HIV seropositive I.V drug Usersand their non infecting wives in Manipur. Indian J. Med. Res. 2000; 111, 37-39.
5. Mukhopadhya A. Hepatitis C in India. J biosci. 2008; 33:465-473.
6. Maticic M, Paljak M, Kramar B, etal. Detection of hepatitis C virus RNA from gingival crevicular fluid and its relation to virus presence in saliva. Journal of Periodontology, 2001; 72(1); 11-16.
7. Sood A,Midha V, Avasthi G. Hepatitis C - Knowledge and practices among the family physicians. Trop Gastroenterol 2002: 23 (4); 198-201.
8. Deepak Arora, Neerja Jindal, Raman Dang, Rajiv Kumar. Rising seroprevelance of HCV a silent killer - Emerging problem.Int J of Pharm Pharm Sci. 2011, 3 suppl 4: 57-59.
9. Coates E.A., Brennan D, Logan R.M, Goss A.N, Scopacasa B, Spencer A.J, etal. Hepatitis C infection and associated Oral Health problems. Aus Dental J 2000;45 (2);108-114.
10. de Mattos Camargo Grossman S, de Aguiar M.C, Teixeira R, do Carmo MA. Oral Lichen Planus and chronic hepatitis C; a controversial association. Am J Clin Pathol 2007; 127(5): 800-4.
|