Introduction
“Occlusion” in very simple terms can be defined as an intercuspal relationship between the set of maxillary and mandibular teeth. But encompassing a broader spectrum, Occlusion is the integrated relationship of the teeth, periodontium, neuromusculature, and not just interdigitation. This relationship is a dynamic entity and can be extremely complex and varied.
A singular concept of occlusion cannot be applied to all patients. This relationship can exist in a variety of forms, and in a state of normalcy and balance, remains in harmony with the other structures , which make up the dento-alveolar apparatus.
Even though, studied exclusively, some aspects of "Occlusion" still eludes us, or rather it can be Said, that the implications of occlusion on multiple number of situations are still not completely understood. Over the years, a number of attempts have been made to put all the parameters of this "intercuspal relationship" into perspective and even though some of these guidelines are very appropriate, there are a number of misinterpreted facts on Occlusion which abound in the literature.
It will be attempted in this article to arrive at some conclusive endpoints, based on a lot of current data which is now available on the subject of "Occlusion". The literature throws up some basic recommendations based on these conclusions as regards carrying out advanced and extensive aesthetic work in the dentition.
Studying Occlusion becomes simpler under the following three situations.
Occlusion in a state of health
Occlusion in a state of ill health
Occlusion as a consideration in aesthetic dentistry
A. Occlusion in a state of health:
A state of health is considered to be true, as far as the dentition is concerned, when the subject has no complaints and a dental examination does not reveal any underlying pathology that is either infective or degenerative in nature in relation with the entire dental apparatus. Once determined, that the oral cavity is in a "state of health" the occlusion can be examined. A look at literature as well as evidence stemming from experience in dental procedures of a number of clinicians, it seems to indicate that the interface between the maxillary and mandibular teeth is very adaptive and can establish itself in a variety of different relationships.
Dental undergraduate students are usually given to understand occlusal relationships in terms of relative positions. One of the most popular forms of classifications of occlusal relations is the "Angles" classification of occlusion. In this classification, three primary divisions have been created, namely class I,class II and class III. The key for the Angle classification, which was created one century ago (1907) by Edward Angle, is the relationship between the upper and lower first molars. It is to be noted at this point, that the relative position of the mandible to the maxilla was recorded during the static condition of "Centric Occlusion".
A healthy, natural Angle Class I occlusion is characterized by simultaneous, equalized contact of all teeth (anterior and posterior) in maximum intercuspation (centric occlusion) (Fig 1 and 2)
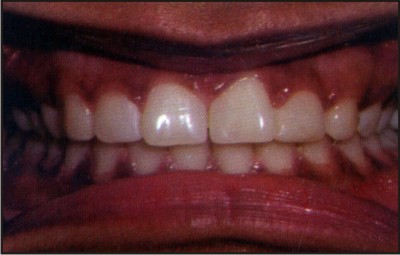 | Fig 1: A typical angles Cl I occlusion
 |
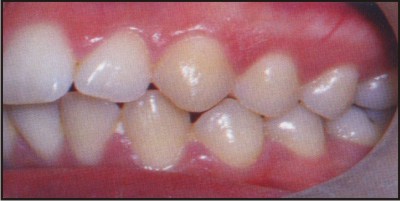 | Fig 2: The cusp to fossa relationship upper/lower premolars and molar
|
This point shall be elaborated later in this article. The Class II group has been further subdivided into Div I and Div II.
It has been observed that the greater majority of the population fall in the classical "Class I" group. In this relation, the maxillary teeth encompass the mandibular teeth circumferentially and the cuspal relationship of the first maxillary molars is in alignment with the mandibular first molar in such a way that the mesio-buccal cusp of the upper first molar rests in the mesio-buccal groove of the lower first molar.
The Class II group has the mesiobuccal cusp of the upper first molar resting anterior to the Class I position and may lie between the lower first molar and the lower second premolar. This has been further sub-divided into two groups.
i. Class II Div I in which the maxillary anterior teeth are protruded.
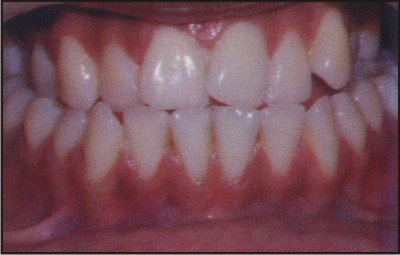
ii. Class II Div II in which the maxillary incisors are retroclined and the lateral incisors overlap the central incisors on the mesial side . (Fig 3)
 | Fig 3: A classical angles Cl II occlusion
|
A Class III occlusion is one in which a reversal takes place and the maxillary teeth are contained In the mandibular teeth and the lower anterior teeth are placed labial to the upper anterior teeth.
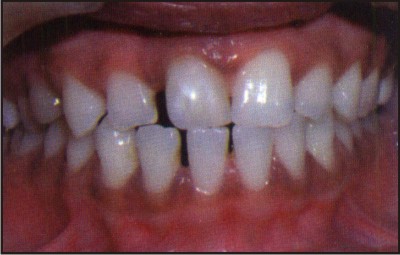
According to Angle , whenever teeth do not follow the above exemplary relationship , they are said to be in a state of "Malocclusion". In fact even a perfect Class I molar relation, if the rest of the teeth do not remain in perfect alignment , it would be considered to be a malocclusion . Over the years, there have been numerous attempts to refine the traditional "Angles" classification and make the groupings more specific and detailed. Additional inputs, other than the basic clinical examination to determine the occlusal position have been included to elaborate the occlusal relationships. These have been the use of the Lateral Cephalogram Radiographic picture which gives extensive skeletal relationship of the maxilla and mandible.(Fig 4)
 | Fig 4 : A classical Angles Cl III Occlusion
|
It must be stressed that most of the radiographic analytic methods have been primarily aimed towards determining and predicting growth patterns and if possible interventional methods to guide the growth in a more desirable and favorable pattern. Even though the Tweed and Bolton analysis (to name a few) of Angles classification are an accepted refinement of the study of occlusal relationships, they have not widened the scope of the occlusion relationship to bring in the elusive factor of "Function".
As dental students, as academic teachers as well as clinicians, we tend to regard "Malocclusion" as a pathological condition. Is this true? Should Malocclusion be considered to be a pathologic entity or should it be considered to be just " Relative positioning of teeth with an aberration from the majority"?
This could be considered to be "Unaesthetic" with the realization that "aesthetics" is a very relative and subjective consideration. We do have classical examples of certain media stars who look so cute and attractive with absolutely out of position, buccally placed canines. On the other hand we also have the handsome and extremely attractive, beautiful faces, which get marred by the minutest of discrepancies of position in the anterior segment.
A look into the literature generates some very interesting findings. Most of the criticism attributed to Angles classification has been that it is very limited in scope and the key factors taken into consideration for classifying "Malocclusion" are not complete. In fact, a few elaborate suggestions involve extensive and detailed skeletal measurements in multiple dimensions.
The Witts modification is one such excellent attempt to analyze the skeletal as well as dental relation with a very scientific method. As late as in 2005, a modification of Angles classification was suggested by A. Pitts in the Journal of Orofacial Orthopaedics1 in which he felt that it was not clinically practical to use the large number of measurements required to classify “occlusal relationships”. He built upon the classical Angles classification refined with almost a 100 years of additional data, to come up with a more practically applicable method of classifying occlusion.
Class I - He has proposed all malocclusions in the antero-posterior plane primarily affecting the maxilla to be grouped as Class I with three subdivisions.
Division 1- Maxillary protrusion
Division 2 - Maxillary retrusion with normal molar occlusion
Division 3 - Maxillary retrusion with secondary mandibular retrusion ( corresponding to Angles Class II, Div 2 )
Class II - This group is characterized by a post- normal relationship of the lower arch to the Upper arch (corresponding to Angles Class II Div 1)
Class III - This group has the lower arch in a mesial relation to the upper arch ( corresponding to Angles Class III)
In fact, the editorial in the Journal of Orthodontics 2 in 2003 very unequivocally states that the
reliance of the Angles classification on the molar relationship is quite incomplete and stresses greater importance on the canine relationship. Even from a pure orthodontic standpoint , basing a case as unaesthetic on the classical Angles system may not be appropriate in the current context.
A step further to be built up on this is the fundamental question if a "malocclusion" is a pathological condition which is deleterious to health and function.
B. Occlusion in a State of Ill Health:
Occlusal relationships can take a dramatic turnaround when the oral cavity is in a state of ill health. Ill health signifies some kind of damage to existing and / or loss of the teeth concomitant with progressive disease in the existing teeth. There are two issues which have to be addressed. The first issue arises out of loss of key teeth in the dentition. If certain key teeth are lost, the transmission of masticatory loads as well as forces generated by any parafunctional habits become very high. This kind of situation is also referred to as secondary trauma from occlusion. The second issue is that of damage to existing teeth. The dentition usually gets mutilated either due to carious destruction or periodontal disease. Either of the two is damaging and leads to a complete change of orientation of transmission of occlusal forces.
Such kind of situations lead to potential realignment of the existing teeth which can lead to further complexities.
C. Occlusion as a consideration in aesthetic dentistry:
The role that occlusion plays in any kind of complex and extensive aesthetic treatment plan is of very high importance and can be one of the sole reasons for a long and successful outcome of the entire therapy. There have been many an instance of a veneers popping off, crowns chipping, incisal edges breaking down as well as complete breakdown of direct bonding restorations.
At times it is baffling as to why certain aesthetic restorative procedures work so excellently and the same amount of diligence and effort does not pay dividends in other cases. The key difference generally is the occlusal relationship of the teeth. The term which is being more and more used now to address this problem is “Occlusal Disease”
“Occlusal Disease” encompasses under its umbrella a variety of different clinical situations which have not always be traditionally attributed to aberrant occlusal forces. It covers the conditions of bruxism, clenching, primary and secondary occlusal trauma afflicting the periodontium, TMD, abfractions and cervical hypersensitivity3.
Discussion:
The clinician will encounter occlusal disease almost on a daily basis, but attempts are usually made to treat the problems symptomatically. There is an immediate transient resolution, but no long term benefit in a large number of cases wherein the root cause is occlusal disease. The essence of occlusal disease is the creation of high stress in localized, isolated parts of the
dentition and the consequential breakdown of these areas due to the inability to withstand the high loads. A common fallacy is to attribute the damage caused by occlusal disease as a natural process of wear and tear of the dentition (Fig 5) .
 | Fig 5: A successful smile design outcome is dependent on the occlusal correction
|
A very excellent system of recording and diagnosing the etiology of unaesthetic conditions has been developed by Dr. Luiz and has been termed as the Dento Facial Esthetic Diagnostic System (DFED). This system requires a detailed record of the entire dentition measuring a number of parameters. It requires a full set of IOPA radiographs, an OPG, detailed periodontal charting, models mounted on a semi adjustable articulator with the transfer done using a Kois face bow and a set of 11 clinical photographs4.
Once the entire occlusal pattern has been recorded, it will be possible to attribute specific unaesthetic symptoms of cervical abfractions, tooth chipping and recession to occlusal disease. The imperative issue is that the esthetic treatment plan has to identify any such etiology of "occlusal disease" and once identified, measures have to be taken for rectification.
Occlusal disease can be corrected by means of very specific and precise equilibration of the occlusion in centric occlusion to create completely balanced and equidistributed occlusal loads. It has to be borne in mind that the equilibration cannot be done completely in one sitting. It will require slow and systematic correction over a number of sittings spread over a few weeks. If the occlusal disease also presents signs of parafunctional habits of bruxing and specifically “clenching”, it is very important to try first of all break the habits ( which is easier said than done -since the pathway of progression of the habit is not clearly understood) and secondly to counter the ill effects of the parafunctional habits5.
This can be achieved by the use of occlusal splints which may have to be modified over time. The Lucia jig is a modification of the occlusal splint. A newer method which has gained considerable grounds over the past few years has been the NTI device which not only helps in these conditions but also is very effective in countering the more severe deleterious effects of the parafunctional habits.
Summary & Conclusion:
In the last, it can be said, occlusion can well be the most critical factor in achieving and establishing aesthetic smiles. Any anterior or for that matter even a posterior restoration or replacement placed as part of the personality change of an individual, has to amalgamate the functional aspect of equilibrated occlusion in centric and during lateral and protrusive movements along with the aesthetics. The adage of the current era could well be " Aesthetics is the form that follows the function of occlusion".
References:
1. A.T.Pitts, Journal of Orofacial Orthopaedics, April 1931, Volume1, Number:2.
2. Editorial, Journal of Orthodontics(British Orthodontics Society ), December 2003,Vol.30, No:4, 279.
3. M.Hisano, K.Soma, Journal of Oral Rehabilitation, October 1999 Volume 26, Issue 10, Page 830-835.
4. Gordon Christensen, Now it's the time to observe and treat dental occlusion, J Am Dent Assoc, Vol 132, No 1, 100-102.
5. Jose-Luis Ruiz, Achieving Longevity in Esthetic Dentistry by the Proper Diagnosis and Management of Occlusal Disease, Contemporary Esthetics & Restorative Practice, June 2007 |