Over the past various attempts have been made to measure the dimensions of face. Attempts were also done to simulate the results of surgery on face and jaws and to predict facial change following surgery.
In the past direct measurements using classical methods of physical anthropology like those using standard anthropometric tools such as sliding calipers, spreading calipers, soft tape and a protractor have been used to access the facial asymmetry. These measurements can be prone to inaccuracies. The commonest sources of error in antropometry are due to improper identification of landmarks, inadequate measuring equipment and improper measuring techniques1.
Morphoanalysis has been used in an attempt to reconstruct the facial form in three dimensions by superimposition of radiographic and photographic material, but the method did not gain wide acceptance.2,3 Later stereoradiographic techniques with metallic implants was used to study the growth of children with congenital anomalies or deformities. Again this technique is limited in its application as metallic markers need to be placed surgically before the recording is made, and there is a cumulative radiation dose to the child.4 Further technique has been developed to use a computer to predict facial form using two dimensional lateral skull radiograph. The data is obtained by moving a digitizing the cursor along the anatomical features in the radiograph. This technique is time consuming, of limited accuracy, and only gives a representation of predicted outcome in the midline. The method does not provide an analysis in three dimensions.5
Previous approaches to obtaining three dimensional facial data included computerized tomography (CT) and (MRI). However, the resolution of facial structures is limited by the separation of CT scans. In addition soft tissue resolution is poor. Both MRI and CT scans also produce distorted facial reconstruction because artifacts are generated by metallic objects such as fillings in teeth. Finally, neither CT nor MRI Provide the natural photographic appearance of the texture of the facial surface.6
All the above mentioned approaches have their limitations, both in radiation dose and in their ability to measure accurately the face and skull in three dimensions. To overcome these difficulties a laser scanning has been designed.
Laser scanning Technique
Patient sits in a rotating chair, opposing camera. A non hazardous line of helium- neon laser light is projected on the face while the chair is rotated. The distorted laser light reflecting the subjects facial anatomy is recorded by the camera with the use of mirrors and is sent to computer and can be retrieved at a later date for further analysis. The hard copy of the laser graph can be printed in full colour or black and white in any required view1 (Fig 1).
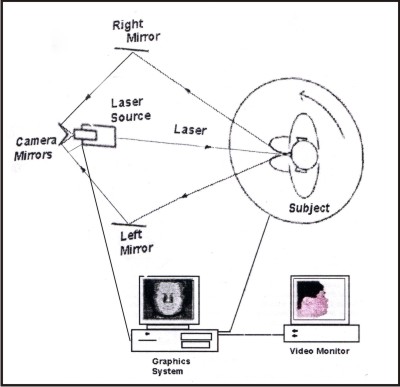 | Fig 1 - Laser Scanning Technique
 |
Assessment of Optimal scanning conditions.
The Frankfort horizontal plane be parallel of the patient and the frontal view axial plane perpendicular, to the true horizontal plane for a reproducible three dimensional laser graph. Best scanning quality was obtained when the subject was centred in the scanner working volume.9
Artefacts
Factors that generated artifacts was conducted empirically and revealed that the most relevant aspects during scanning were the laboratory environment, facial surface conditions and motion artifacts.
The precautions required to reduce the artifacts were- completely darkening the room, removing or masking any object in the room that had a reflective surface. All the situations that modify the skin texture and alter refraction (ie sweat, hydration or creams) appeared a possible cause of artifacts in the acquired data. Carefully cleaned facial skin and climate control were thus required for the examination.
The most common source of artifacts was subject motion during the time required to complete digitization. Motion may affect a part of the face, most commonly owing to eye movements or facial expressions, or it may affect the whole head because of trembling of neck musculature. In all subjects, the best examinations were obtained when the patient was allowed to keep the head in a natural relaxed position; forcing head flexion or extension exacerbated trembling.9
Evaluation of scanning errors.
The accuracy of scanning was +/-0.65mm. The development of a specific protocol resulted in a mean scanning error of 1-1.2mm and a recording error of 0.3-0.4mm on repeated scans of human subjects.9
Precision and Accuracy
The reported precision of the laser scanner has been assessed as 0.6-2mm on plaster head models depending on the use of Prelabelled landmarks.10 Accuracy for point localization on human subjects, in comparison with direct anthropometric measurements was determined to be with in 1.5 mm for only one third of the most commonly used measures, and unreliable (>2mm) for the other two thirds. The accuracy of the laser scanning in the study by Ramieri et al appears to be high when compared to CT Scans.11
Discussion
I.J Coward et al (1997) carried out Laser scanning on ears and face. And concluded that the siting of the landmarks in a image captured by this technique has been shown to be in accurate in identifying landmarks of ears and face and suggested that if landmarks can be consistently sited on a laser scan image, they would then be able to be used to calculate dimensions of an ear and its location on face.1
Moss J P et al (1987) described the use of a specially designed no contact laser scanning system and CT for studying changes in the facial form and its relationship to changes in the supporting bone structure after facial surgery. It is shown that realistic images may be produced from these data sets using computer graphics techniques to give the images a solid 3D appearance. The images may then be used for planning surgery and to provide the patient with a prediction of facial appearance after surgery.12
Patch work in the form of triangles or facets from CT or Laser contoured data from CT
Computer graphics techniques
Image is shaded and illuminated to provide realism (Fig 2)
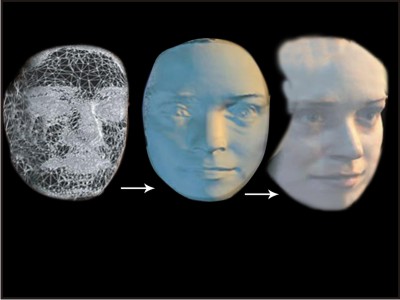 | Fig 2 - Image Formed Using Laser
|
The faceting technique is not suitable for applications to the complicated surfaces of the skull. The skull, therefore treated as a series of volume elements, called voxels. Several methods can be used to display voxels, most frequently used is Octree encoding (Meagher, 1982)13. The principle is to define a three dimensional array of cubical array.
Surgical simulation may be performed interactively on the skull by selecting volumes of interest which may be repositioned, removed, rotated or added to, then redisplayed in any chosen orientation. Models for predicting the behaviour of the soft tissue after the alteration of the underlying bone structure are being developed to give some indication of the effect of surgery on facial appearance. The graphics techniques described enable the patient to be presented with a picture of the effects of surgery on face in three dimensions before surgery is undertaken. It is also a valuable asset to the surgeon who is able to identify and view the morphology of the bone within the maxilla or the base of the skull to determine the areas where surgical intervention is necessary. An accurate method of measuring and visualizing the face and skull in three dimensions has been described, and its use in the treatment of the patients with congenital facial deformity has been reported.12
Reliability of a 3D surface scanner for orthodontic applications.
Budi Kusnoto et al (2002) assessed the reliability of generating 3D object reconstruction using the Minolta VIVID 700 3D surface laser scanner. Accuracy & Reproducibility were tested on a geometrical calibrated cylinder, a dental study model and a plaster facial model. Tests were conducted at varying distances between object and scanner. In calibrated cylinder tests, spatial distance measurement was accurate to 0.5mm (+/-0.1mm) in vertical dimension & 0.3mm (+/-0.3mm) in horizontal dimension. In study model test molar width was accurate to 0.2mm and palatal vault depth could be measured to 0.7mm. For facial model, an accuracy of 1.9+/-0.8mm was obtained. These findings suggest that the surface scanner has great research potential because of accuracy and ease of use. Treatment changes, growth, surgical simulations and many other orthodontic applications can be approached 3 dimensionally with this device.
The self corrected mechanism of the laser scanner in adjusting for image distortion gives flexibility for clinical research. The software can be used to merge images taken from different perspectives, thus eliminating undercuts. Interestingly due to laser beam spread, it was found that the smaller the object, the more accurate measurements. For craniofacial anomalies, various studies could be performed regarding cleft lip repair, asymmetric facial growth, change of head shape& nasal molding procedures.14
Advantages
One of the major benefits of this system is the facility to manipulate the image in three dimensions. Thus, one can rotate the image on the computer screen in any direction and angle and select points on a standard or customized reference plane.8
All anatomical landmarks and facial structures are recorded with in 0.5mm, which meets the current clinical requirements of accuracy and reproducibility for orthognathic surgery assessment and treatment planning12.The method can be repeated without danger to the patient and has high spatial resolution and does not involve contact with the patients face. It can therefore be used for longitudinal studies of soft tissue changes in growing individuals and following surgery. This information is used together with a low dose CT scan to provide information on the bone structure and its relationship to the soft tissue. This method also provides realistic three dimensional imaging of the face and skull.15
Conclusion
Three dimensional surface digitization through laser scanners offers excellent possibilities for objective analysis of the human face. Many more applications are possible in studying facial soft tissue growth, functional facial muscle movements, dental casts, arch form and head shape. Hence, laser scanning has to be studied and all possibilities for the various research techniques to yet be explored.
Bibliography
1. Coward TJ, Watson RM, Scott BJJ. Laser scanning for the identification of repeatable landmarks of ears and face. British Journal of Plastic Surgery. 1997; 50:308-314.
2. Rabey GP, Craniofacial morphanalysis. Proceedings of the Royal Society of Medicine. 1971; 64:103-111.
3. Rabey GP, Current Principles of morphanalysis and their implications in oral surgery Practice. British journal of Oral surgery 1977; 15: 97-134.
4. Rune B, Sarnas KV, Selvik G. Roentgen stereometry with the aid of metallic implants in hemifacial microsomia. American journal of Orthodontics 1982; 81: 65-70.
5. Harradine NW, Birnie DJ Computerised prediction of the results of orthognathic surgery. Journal of Maxillofacial Surgery 1985; 13: 237-245.
6. Hoenhen KH, Hanson WA. Interactive 3 D Segmentation of MRI & CT volumes using morphological operations. J Comput Assist Tomogr 1992; 16: 285-294.
7. Ayoub AF, Siebert P, Moos KF, Wray D, Urquart C, Niblett TB. A vision - based three dimensional capture system for maxillofacial assessment and surgical planning. British journal of Oral & Maxillofacial Surgery. 1998; 36: 353-357.
8. Soncul M, Bamber MA. The reproducibility of the head position for a laser scan using a novel morphometric analysis for orthognathic surgery. Int. J. Oral Maxillofac surg 2000; 29: 86-90.
9. Ramieri GA, Spada MC, Nasi A, Tavolaccini A, Vezzetti E, Tornincara S, Bianchi SD, Verse L. Reconstruction of facial morphology from Laser Scanned Data Part 1; Reliability of technique. Dentomaxillofacial Radiology 2006; 35:158-164.
10. Bush K, Antonyshyn O Three dimensional facial anthropometry using a laser surface scanner, Validation of technique. Plast Reconstr Surg 1996; 98:226-35.
11. Aung SC, Ngim RC, Lee ST. Evaluation of the laser scanner as a surface measuring tool and its accuracy compared with direct facial anthropometric measurements. Br J Plast Surg 1995; 48: 551-558.
12. Moss JP, Linney AD, Grindord SR, Arridge SR, Clifton JS. Three dimensional visualization of the face and skull using computerized tomography and laser scanning techniques. European Journal of Orthodontics 1987; 9:247-253.
13. Meagher D. Geometric modeling using Octree encoding. Comput Graph Image Poc 1982; 19:129-147.
14. Kusnoto B, Evans CA. Reliability of 3D Surface laser scanner for Orthodontic applications. Am J Orthod Dentofacial Orthop 2002; 122:342-8.
15. Girod S, Keeve E, Girod B. Advances in interactive craniofacial surgery planning by 3D simulation and visualization. Int J Oral Maxillofac Surg 1995; 24:120-5 |