Introduction
Resorption of alveolar ridge, a common physiological finding after tooth loss, often requires periodontal corrective surgery before prosthetic, and implant placement.1 Especially in the anterior visible region ridge collapse leads to unacceptable structural, functional and above all esthetic compromises. From a morphologic standpoint, Seibert classified ridge deformities into three types according to the vertical and horizontal defect components2
1. Class I defect
Buccolingual loss of tissue contour with a normal apicocoronal height.
2. Class II defect
Apicocoronal loss of tissue with normal buccolingual contour.
3. Class III defect
A combination of buccolingual and apicocoronal loss.
Later, Allen et al.3 introduced severity as a classification criterion in the evaluation of alveolar deformities. Severity is classified as-
Mild deformity < 3mm
Moderate deformity 3 - 6mm
Severe deformity > 6mm
Ridge augmentation is a valuable periodontal plastic surgery procedure for correction of ridge defects for esthetic purpose. Soft tissue ridge augmentation using palatal grafts have been thoroughly documented in the management of residual ridge deformities. The technique that have been used for this purpose are Roll flap procedure4, Pouch graft procedure 5, onlay epithelialized grafts 6, interpositional graft technique7, and combined onlay interpositional graft8 procedure.
In this case report we augmented a alveolar ridge by the pouch technique using subepithelial connective tissue graft combined with bone graft.
Case Report
A 45 Years female patient reported in the Department of Periodontics, Institute of Dental Sciences, Bareilly, with a complain for unaesthetic tooth site. She stated that following removal of upper left central incisor, the site healed with a deep notch in the gums. Intraoral examination revealed a mild to moderate buccolingual ridge deficiency in missing tooth region, leading to the diagnosis of class I alveolar ridge defect (Fig. 1, 2). Patient had no systemic abnormality. On discussing the condition and findings, she agreed for soft tissue ridge augmentation procedure followed by prosthetic replacement. Thorough scaling and root planning was given to the patient for removal of the local debris, and patient appointed for surgical phase after 1 months.
 | Fig. 1 - Facial View Of Class I Alveolar Ridge Defect
 |
 | Fig. 2 - Occlusal View Of Class I Alveolar Ridge Defect
|
Surgical Procedure
After administering local anesthesia, incision was given for pouch formation on the alveolar crest in the buccal side of involved area (Fig. 3). This pouch was extended in the apical aspect of alveolar ridge for adequate depth with the help of periosteal elevator. Subepithelial connective tissue graft was harvested from the palatal aspect of left second premolar region (Fig.4,5). This connective tissue graft transferred to the preformed pouch that was filled with decalcified freeze dried bone allograft (DFDBA) (Fig. 6, 7). After suturing, the site was covered with periodontal pack. Postoperative antibiotics, analgesics, and 0.12% chlorhexidine mouth rinse for 7 days were prescribed to prevent any postoperative discomfort. After 7 days, periodontal pack, and sutures were removed. The surgical site was found to heal without any complication (Fig. 8). At 21 days, and 3 months postoperative follow-ups, there is uneventful healing, and no decreased in tissue volume was noticed (Fig. 9, 10). The patient was instructed to maintain proper oral hygiene and referred to Prosthodontist for prosthetic requirements.
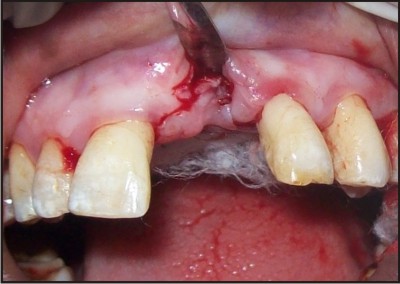 | Fig. 3 - Pouch Formation In Involved Site
|
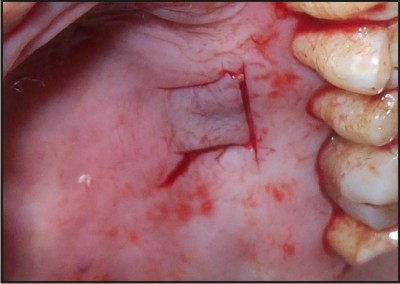 | Fig. 4 - Site Of Connective Tissue Harvesting
|
 | Fig. 5 - Subepithelial Connective Tissue
|
 | Fig. 6 - Bone Graft In Pouch
|
 | Fig. 7 - Connective Tissue And Suturing
|
 | Fig. 8 - Uneventful Healing After Surgery
|
 | Fig. 9 - After 21 Days, Uneventful Healing
|
 | Fig. 10 - Increase In Buccolingual Width After 3 Months
|
Discussion
A deform ridge may result from tooth extractions, sever periodontal disease, abscess formations, etc.1 The deformity that exits in the ridge is directly related to the volume of the root structure and associated bone that is missing or has been destroyed. Several soft tissue augmentation techniques have been developed to reestablish natural appearing soft tissue architecture. The following factors should be determined prior to the initiation of therapy-
Volume of tissue required to eliminate the ridge deformity
Type of graft procedure to be used
Timing of various treatment procedure
Problem with tissue discolorations and matching tissue color.
Roll flap technique involves the preparation of a de-epithelialized connective tissue pedicle graft, which is subsequently secured in a subepithelial pouch for deformity correction. This procedure is used for small to moderate class I ridge defects in localized area. A depithelialized palatal connective tissue pedicle flap removed from the adjacent site of collapse ridge, and tucked into the buccal gingival pouch. A pouch is made in the supraperiosteal connective tissue at the labial surface of the ridge. The result of this procedure may be satisfactory but technique may not be convenient due to anatomic considerations and finite tissue thickness.4
Pouch graft procedure is used for class I type alveolar ridge deformity. For this type of augmentation a subepithelial pouch is prepared in the area of the ridge deformity, into which a free graft of connective tissue is placed and molded to create the desired contour of the ridge. We have used bone graft (DFDBA) combined with connective tissue harvesting for the pouch technique. Connective tissue grafts give excellent color match of the surrounding tissue, and due to good blood supply they are well received by the recipient site.5
Onlay graft are epithelialized free graft, which following placement, receive their nutrition from the de-epithelialized connective tissue of the recipient site. This type of graft is use for large class II and III defects. If necessary, grafting can be repeated at 2-3 months intervals to gradually increase the ridge height. Onlay graft maintains their epithelium over the connective tissue. The graft is secured with its connective tissue base in contact with de-epithelialized recipient site. Significant ridge correction can be achieved by this technique, but due to color difference between from palatal and gingival tissue, it may create unpleasant esthetic results. 6
Interpositional grafts are used to correct class I, and mild to moderate class I and II defects. The surgical procedure requires the use a thick, wedge shape connective tissue graft. This graft is then inserted in the recipient bed, creates similar to the pouch procedures by means of partial thickness dissection. The graft is sutured, leaving the epithelial surface at the level of surrounding tissue. 7
Combined onlay interpositional graft attempt to maximize the benefits of onlay epithelialized graft and subepithelial connective tissue graft. This type of augmentation is mainly used for class III ridge defects. The submerged connective tissue section of the interpositional graft aids in the revascularization of the onlay section of the graft, thereby gaining a greater percentage of success of the overall graft.8
Different surgical techniques have shown acceptable esthetic outcome. Nevertheless, many of these results are case reports or series, and outcome are mainly related to skill of the operator. Generally the published cases show short term results. Long term stability of the regenerated tissues should be proven in longitudinal studies.
Conclusion
This article demonstrates the correction of an unaesthetic ridge deformity using pouch technique. The pouch method provided adequate volume to establish natural appearing soft tissue architecture. This technique facilitates the ease of graft placement and aesthetic result.
References
1. Schropp L, Wenzel A, Kostopoulos L, et al. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003;23:313-323.
2. Seibert JS. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts: I. Technique and wound healing. Compendium of continuing education in general dentistry 4,437-453.
3. Allen EP, Gainza CS, Farthing GG, Newbold DA. Improved technique for localized ridge augmentation. A report of 21 cases. J Periodontal. 1985;56:195-199.
4. Scharf DR, Tarnow DP. Modified roll technique for localized alveolar ridge augmentation. Int J Periodontics Restorative Dent. 1992:12:415-425.
5. Langer B, Calanga L. the subepithelial connective tissue graft. J Prosthet Dent. 1980;44:363-367.
6. Seibert JS. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing.Compend Contin Educ Dent. 1983;4:437-453.
7. Seibert JS. Treatment of moderate localized alveolar ridge defects: preventive and reconstructive concepts in therapy. Dental Clinica of North America 1993a;37,265-280.
8. Seibert JS, Louis JV. Soft tissue ridge ridge augmentation utilizing a combination onlay interpositional graft procedure: a case report. Int J Periodontics Restorative Dent. 1996;16;310-321. |