Introduction
Successful implant treatment is directly related to achieving integration and restoring hard and soft supporting structures for esthetics and function [1].Itis necessary for the clinician to visualize the final prosthetic result before implant placement and to have thorough understanding of the surgical and prosthodontic phases of treatment to achieve a predictable outcome[2].This desire of predictable results led to development of prosthetically guided implantology. Despite significant advances in devices and techniques, placing dental implants in a correct position still remains a challenge. Diagnostic casts, probing depths and panoramic radiography can lead to unpredictable results as they do not give three-dimensional (3-D) radiographic information required for correct positioning and orientation of implant [1]. Moreover, implant supported prosthesis requires determination of final prosthesis during treatment planning stage. Thus for a successful implant supported prosthesis the Prosthodontist should plan the implant position in accordance with accurate mesiodistal and buccolingual location, angulation with residual bone and correct implant orientation. To achieve these objectives dental CT scan imaging in conjunction with radiographic guide (stent) with radiopaque marker should be used.
Surgical stent provides communication between the surgeon and restoring dentist, so that the implant is placed at the ideal position and angulations The purpose of stent is to preview the definitive restoration and its relationship to adjacent structures, to communicate the restoration planned by the Prosthodontist to the surgeon, to reduce osteotomy and to locate healing screws at the time of second stage surgery [3].
This article features a method of using existing mandibular complete prosthesis as radiographic stent and a duplicated denture as a surgical template. Advantages of the technique are twofold: it is cost effectiveand makes use of equipment and materials commonly found in dental clinics.
Case Report
A 54 year old male patient reported to Department of Prosthodontics with complaint of loose mandibular denture.Clinical and radiographic examination revealed adequate maxillary bone height and anteriormandibular ridge resorption. Evaluation of existing dentures revealed adequate extensions with fair amount of retention and stability along with satisfactory position of denture teeth. A treatment plan was prepared after a standard protocol that took into consideration patient's desires, treatment alternatives and treatment costs. The plan included fabrication of conventional complete dentures for maxilla and an implant retained overdenture for mandibular arch.
For diagnostic preoperative evaluation, patient existing denture was used as aradiographic guide. The desired implant locations were marked on existing denture at five positions.In the transverse plane, it corresponds to the interproximal area between the mandibular central incisors,between canine and first premolar and as well as fifth site being in between the first two sites ,on both sides ( Figure 1). Gutta-percha cones were used as radio opaque markers to the mandibular denture to assess the anatomy of proposed implant sites in the denta scan. Denta scan was taken with complete denture acting as radiographic guide in patients mouth (Figure 2,3). After analyzing the denta scan, three implants in mandibular anterior region were planned for the present case.
 | Fig 1 : Gutta Percha Markers Placed At Proposed Implant Sites On The Existing Mandibular Denture
 |
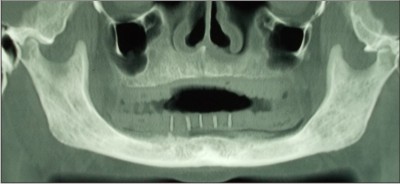 | Fig 2 : Denta Scan With Radiographic Markers
|
 | Fig 3 : Denta Scan With Radiographic Markers
|
For the fabrication of surgical guide template, the patient's mandibular denture was duplicated in duplicating flask by using irreversible hydrocolloid (Figure4). The mandibular denture was stabilized by wax stopper corresponding to access holes in duplicating flask. Irreversible hydrocolloid was used to invest the denture in the flask.After the setting of hydrocolloid, the denture was taken out of the flask. Auto polymerizing acrylic resin was then poured through access holes in the mold and flask was then bench pressed. The mandibular denture wasretrieved from the flask after 30 minute (Figure5) and thereafter finishing and polishing was done ( Figure6,7). This duplicate denture was modified for surgery by creating window like openings at the proposed implant sites to be used as surgical guide template (Figure8). The interproximal positions of gutta-percha were taken as the reference positions.
 | Fig 4 : Self Cure Resin Poured In Duplicating Flask
|
 | Fig 5 : Duplicated Denture While Retrieving From The Flask
|
 | Fig 6 : Duplicated Denture
|
 | Fig 7 : Duplicated Denture
|
 | Fig 8 : Duplicated Denture As Surgical Guide Template Intraorally
|
Discussion
The ability to restore an edentulous arch with endosteal implants revolutionized dentistry. This resulted in a paradigm shift and opened up numerous approaches to restore edentulous arches. As implant dentistry is evolving towards accelerated treatment protocols, with immediate or delayedfunctional and nonfunctional loading, the importance of presurgical planning becomes paramount. Theparadigm for restorative-driven implant placement works best when templates are used to transferinformation from the desired plan to the surgical reality. The advent of computed tomography (CT)imagingand surgical templates allow for clinically significant improvements in accuracy,time efficiency and reduction in surgical error.
This patient was a long term denture wearer with complaint of poorly fitting lower denture. After thorough clinical and radiographic examination ,it was decided to support the mandibular denture with implants. The denta scan is mandatory for such patients which gives a 3-dimensional picture of alveolar bone. Radio opaque Guttapercha markers placed in the existing mandibular denture, helped to assess the anatomy of bone at the proposed implant sites in the patients via the dentascan.
Surgical guide stent is useful for determining the location and direction for fixture installment and can also be used during second stage surgical procedure to identify the position of buried fixture as ideally as possible in relation to residual alveolar ridge[4].
The stents fabricated with the radiopaque markers provide radiographic as well as clinical ease for optimum implant installation. Along with all these advantages, they also provide liberty to flapless implant placement. The drill holes can directly be made through the stent, so the implant surgery may become less traumatic (with the preservation of soft tissue including the gingival margins of adjacent teeth and the interdental papilla) with decreased operative time .This results in accelerated post-surgical healing, fewer post-operative complications and increased comfort and satisfaction for the patients[5].
The foremost advantage of the stent used in this case is its surgical ease, simplicity, precise accuracy and low cost. It can be fabricated with minimum laboratory procedures which are used in routine dental practice. On the other hand, the fixed type screw retained implant stents which are fabricated with the help of CT and CAD/CAM technology are very costly and require more time and laboratory procedures.
In the present case,the stent was made after duplication of the existing mandibular denture by using irreversible hydrocolloid,duplicating flask and self cure acrylic resin. The use of the mentioned materials and equipment made it a verycost effective,quick and easy technique of fabricating surgical guide template
Summary
There is no substitute for thorough diagnosis and treatment planning and meticulous surgical and prosthetic treatment for success of implant supported prosthesis. Proper utilization of surgical and radiographic stents is one of the most important aspects of pre surgical phase.The stent facilitates the accurate placement of implants in optimal positions where sufficient bone is present. In cases with insufficient bone, stent may help in making a strategic alteration of chosen implant site[6]. The use of radiographicstentseither derived from existing prosthesis or from diagnostic wax ups is essential. The incorporation of suitable radiographic markers provide both the surgeon and the prosthodontist with reference points to determine the available bone at theexact spatial location of surgical implant sites[7].
The anterior mandible often shows progressive ridge resorption in the period of edentulousness. Surgical stents help to solve these problems.Using a template ,the accuracy of the proposed direction of implant placement is as close to 5 degree[7].
References
1. Edward M. Armet. Implant treatment planning using patient acceptance prosthesis, radiographic record base and surgical templatePart 1 :Presurgical phase. Implant Dent 1997 ;6:193-`197
2. McCall ra rosenfeld AL. Influence of residual ridge resorption pattern on implant fixture placement and tooth position Part II Presurgical determination of prosthesis type and design. Int J Periodont Rest Dent 1992:12:33-51.
3. Gregori M. Kurtzman, Douglas Dompkowski.Simplifying Implant Surgical Stents for the Partially Edentulous Arch .Inside Dentistry .July/ August 2009,Vol 5,Issue 7.
4. Arun M.L .Optimal placement of osseointegrated implants. J.Cand Dent Asso. 1990; 56(9):8736.
5. U S Pal, Pooran Chand, Neeraj K Dhiman,Singh R K, Vimlesh Kumar. Role of Surgical Stents in determining the positions of implants. National Journal of Maxillofacial Surgery, 2010; 1: 20-23.
6. Naitoh M, Arji E,Okumara S, Onsaki C, Kurita K, Ishigomi T. The use of multiplaner reformatted computerized Tomographyin the surgical prosthodontic planning of implant placement. Clin Oral Implants Res. 2000;11:409-14.
7. Adrian ED, Ivanhoe JR, Krantz WA.Trajectory surgical guide stent for implant placement. J Prosthet Dent 1992; 67: 687-91. |