Introduction
A large number of patients with surgically resected maxillas report to Department of Prosthodontics of various Hospitals for prosthodontic rehabilitation. Such rehabilitation is often a challenging experience for both the operator as well as the patient. The role of both prosthodontists and surgeons has been clearly established. Post-surgical experience of the patient is physically challenging andpsychologically demoralizing .1Maxillary jaw resection often leads to impairment in appearance, mastication, speech, deglutition and self-image, impacting the quality of life of patients so afflicted. Speech of such patients is unintelligible.2
Main objective of prosthetic obturation is closure of the maxillary defect and separation of the oral cavity from sino-nasal cavities. In addition obturator restores function and esthetics, preserves the associated structures and contribute to the patient's perception of improved quality of life. A successful prosthetic design to enable prosthesis function properly utilizes remaining palate and dentition to maximize retention, support and stability of the obturator.
Patients also experience seepage of nasal secretions into the oral cavity, poor lip seal, xerostomia, exophthalmos and diplopia. Acceptance of the new prosthesis is always a slow and difficult process. Patient education plays an important role in the rehabilitation process.
Aramany proposed a defect classification system that presents differences of mechanics in 6 classes that are recognized for prosthetic design of an obturator framework for partially edentulous cases.3,4 A definitive obturator has two components, a metallic framework and an acrylic resin obturator bulb.
The metallic framework stabilizes anticipated cantilever forces along fulcrum line whereas the remaining teeth and the palate provide stability to the prosthesis during mastication and speech.5,6 The intimate contact of the obturator bulb with soft tissues lining the defect not only stabilizes the prosthesis but also minimizes nasal leakage and hyper-nasal speech.
Case Report
A 36 years old male patient reported to the Department of Prosthodontics, Bhojia Dental College and Hospital,Baddi with chief complaint of a large gap due to missing teeth and a portion of the upper jaw bone on the right side [Fig 1]. His medical history revealed that hemi-maxillectomy was performed 2 years back due to a growth in the maxillary sinus.
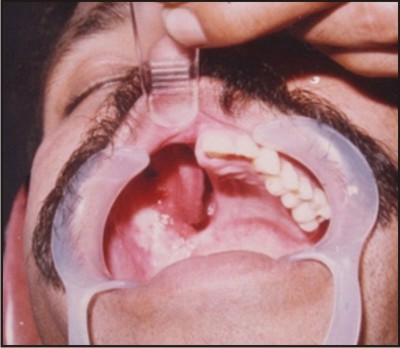 | Figure 1 : Intra Oral View Of The Defect
 |
Facial asymmetry due to collapsed right maxillary region was seen during extra oral examination.Intraoral examination revealed the loss of the alveolar ridge with teeth, hard and soft palate, anterior wall of maxillary sinus and considerable portion of the nasal septum. The defect was classified underAramany class II, as the dentition and the alveolar bone were removed along the midline. The individual had been wearing an ill-fitting acrylic obturator for the past 1 year. Lower jaw and dentition was intact.
The primary aim of the treatment was toseparate sino-nasal and oral cavities to aid in articulation, deglutition, restoration of mid facial contour and improvement of masticatory function.
It was decided to fabricatethe prosthesis in two phases. Firstly the construction of the hollow bulb obturator followed by removable cast partial denture providing support to it.
Procedure
Impressions of the upper and lower jaws were made with irreversible hydrocolloid impression material in stock tray after blocking out the undercuts in the defect area with petrolatum-laden gauze pieces.
Diagnostic casts were obtained. Maxillary diagnostic cast was surveyed and necessary block out was carried out.The defect was outlined and special tray was fabricated on the diagnostic cast using auto polymerizing acrylic resin.
Rest seats were prepared on theteeth 24, 25 and 26. [Fig 2 & 4]
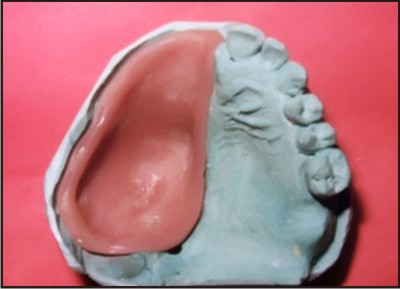 | Figure 2 : Inside View of Hollow Obturator
|
 | Figure 3 : Try in of Cast Metal Framework
|
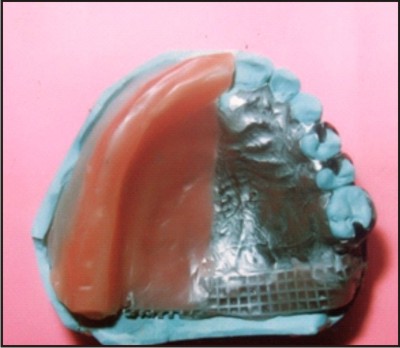 | Figure 4 : Cast Frame Ready for Jaw Relation Record
|
The defect was border molded to record the functional anatomy of buccal and labial tissues surrounding the defect. To make the final impression, gross extent of the defect was recorded using putty material and light body addition polyvinyl siloxane impression material.
The impression of the defect thus obtained was picked up in the stock tray using putty polyvinyl siloxane impression material.
The master cast was obtained from the above impression of the maxillary arch. [Figure 6].
The arbitrary block out of master cast was done and 2 mm thickness of wax build up done to provide adequate thickness of heat cure acrylic resin for strength of the obturator and for construction of hollow bulb obturator portion [Fig 2].
The hollow obturator was fabricated in heat cure acrylic resin comprising main body and lid, which were joined later on with self-polymerizing acrylic resin.
The master cast was then duplicated and refractory cast was obtained on which wax-up for metal framework was done.
The pattern was cast in cobalt - chrome alloy. After finishing and polishing, a metal try in of the framework was done [Fig 3 & 4].
Wax bite block was fabricated on the metal meshwork portion ofthe denture base framework overlying the defect site[Fig 4].
A jaw relation record was made and casts mounted on asemi adjustable articulator for the teeth arrangement.
After the try in, the denture was processed in heat cure acrylic resin[Figure 5].
The hollow bulb obturator shell and the denture were joined using auto polymerizing acrylic resin.
Obturator prosthesis was placed inside the mouth. Patient's speech showed immediate remarkable improvement.
The post insertion follow up and the patient care were carried out at the prescribed intervals of time.
Patient was extremely comfortable with the prosthesis when review examination was carried out. [Figure 6]
 | Figure 5 : Palatal View of Obturator
|
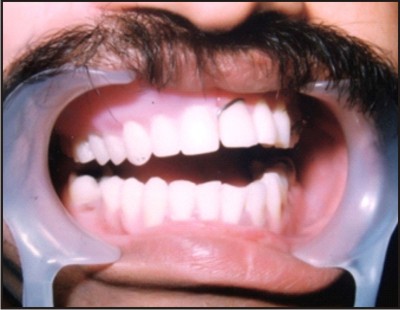 | Figure 6 : Post Insersion View of The Patient
|
Discussion
Comprehensive treatment planning is necessary to meet objectives for patients with complex rehabilitative needs, hence it is necessary to facilitate and coordinate treatment planning among surgeons and prosthodontists.
A range of options is available to the surgeons and prosthodontists for palatomaxillary reconstruction as well as prosthodontic rehabilitation.
A maxillectomy defect in a vertical orientation has a more profound effect on prosthetic stability.
The most important factor for the stabilization of obturator prosthesis is favourable distribution of force during mastication and function. The engagement of structures within the defect diminishes the counterproductive lever forces placed on the obturatorleading to better support, stability and retention of the prosthesis, and thus increasing its success.7
The obturator planned for the patient consisted of two components; a metallic framework and an acrylic resin obturator bulb.
The framework was designed by selecting the most suitable components to resist the various forces acting on the prosthesis without applying undue stress on the remaining teeth and soft tissue structures. The important considerations in designing of the framework were the size and the location of the defect as they relate to the remaining palate and dentition. Maximum support was planned through utilization of full palatal coverage. Preservation of teeth or part of the residual ridge across the midline greatly improved obturator stability. Tissue ward movement was resisted by placement of multiple occlusal rests. Retainers and bracing components were designed to reduce the stresses transmitted to the abutment teeth while retaining the obturator in place. The bulb portion was made hollow so as to minimize the weight of the obturator. This improved cantilever mechanism of suspension and avoided stresses on the supporting structures.8 The closed hollow obturator prosthesis can prevent fluid and food collection, reduce air space and allow for maximum extension.9 The buccal wall of the nasal extension was extended superiorly to help resist rotational forces on the abutment teeth. Increasing the height of lateral wall of obturator above the scar band created a longer lever arm from the point of rotation leading to less vertical displacement. Obturator stability was enhanced by maximum extension in all directions.10
Summary
Fabrication of a functional maxillofacial prosthesis requires full application of the clinician's knowledge and experience based on the sound knowledge of principles of RPD design along-with a specific treatment plan.The technique presented allows application of sound prosthodontic principles and judicious design providing effective restoration of function and esthetics in a case involving post-surgicalmaxillectomy defect and its rehabilitation with a hollow obturator.
References
1. Didier M. New surgical obturator prosthesis for hemi maxillectomy patients. J Prosthet Dent 1993;69:520-3.
2. Majid AA. Weinberg B. Speech intelligibility following prosthodontics obturation of surgically acquired maxillary defect. J Prosthet Dent 1979;32:87-96.
3. Aramany MA. Basic principles of obturator design for partially edentulous patients. Part 1:classification. J Prosthet Dent 1978;40:554-7.
4. Aramany MA. Basic principles of obturator design for partially edentulous patients. Part II: design principles. J Prosthet Dent 1978;40:656-62.
5. Brown KE. Peripheral consideration in improving obturator retention. J ProsthetDent1968; 20:176-81
6. Schwartzman B,Caputo A, Beumer J. Occlusal force transfer by removable partial denture designs for a radical maxillectomy. J Prosthet Dent 1985;54:397- 403.
7. Devin JO, Daniel B, Mark U. Prosthodontic guidelines for surgical reconstruction of the maxilla: A classification system of defects. J Prosthet Dent 2001;86:352-63.
8. Ronald P.DesJardius. Obturator prosthesis design for acquired maxillectomy defects. Prosthet Dent 1978;39:424 - 35
9. Barry HH, Carl FD. Fabrication of a closed hollow obturator. J Prosthet Dent 2004;91:383-5.
10. Brown KE. Clinical considerations in improving obturatortreatment .Prosthet Dent 1970; 24 : 461-6 |