Introduction:
Agenesis of some teeth is referred to as hypodontia which is preferable to term partial anodontia. Anodontia, which implies complete failure of the teeth to develop, is a rare condition. The term Oligodontia is sometimes used when only a few teeth are present.1 Stewart states; Oligodontia is the agenesis of numerous teeth (more than 6 teeth) excluding the third molars. Various terminologies are used to describe the congenital absence of teeth in the deciduous and permanent dentition. Hypodontia is used to describe the absence of one or few teeth, oligodontia is used for agenesis of numerous teeth and anodontia is the extreme of oligodontia where there is total absence of any dental structure.2 The condition such as Oligodontia is often associated with specific syndrome &/or severe systemic abnormalities, whereas anodontia is commonly seen in severe cases of ectodermal dysplasia.2, 3
The cause for congenital absence of teeth could be due to any of the following reasons:
1) physical obstruction or disruption of the dental lamina,
2) space limitation, and functional abnormalities of the dental epithelium
3) Failure of initiation of the underlying mesenchyme.
Characteristic dental symptoms associated are reduced number of teeth, reduction in tooth size, anomalies of tooth form, and delayed eruption. The absence of teeth in young patients can cause aesthetic, functional, and psychological problems particularly if the teeth of the anterior region are involved .2, 3
Case Report:
A 15 year old female patient reported to a private clinic, with a chief complaint of missing teeth in the lower front tooth region. The intra oral examination showed the presence of following permanent teeth i.e. 16 , 12 ,11 and 21, 22,24,25,26 in the maxillary arch and 34,35,36 37, 44, 45,46 in the mandibular arch. The teeth clinically absent were15,14,13,23, 31,32, 33, 41,42,43 in both the arches. Retained primary teeth were 54, 55 and root stump of 72, as seen in Fig [1 to 4 ].
 | Fig 1. Teeth present in upper arch are 16, E, D, 12, 11,21,22,24, 25 and 26
 |
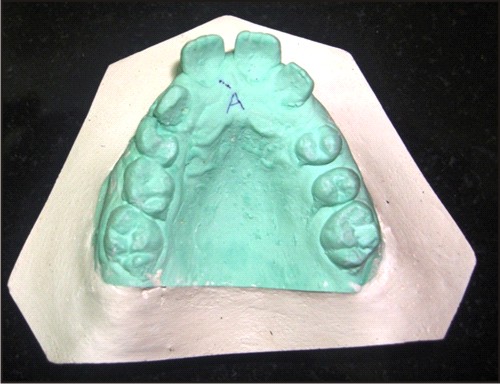 | Fig.2 Maxillary cast teeth present 16,E,D,12,11,21,22,24,25,26
|
 | Fig.3 Teeth missing in the lower anterior region 31, 32, 33, 41, 42, and 43, also note the root stump of 72, i. e. Left lower B
|
 | Fig.4 Mandibular cast with Permanent teeth present 37,36,35,34, 44, 45, 46 and the teeth in the anterior segment are missing
|
The examination of soft tissues revealed no significant abnormality. The dentition of the parents and sibling were normal. There was no history of any infection or trauma to the anterior segment. According to the past dental history given by the patient's mother, the permanent teeth in the mandibular anterior region did not erupt after the exfoliation of the primary teeth. Patient was healthy with no relevant medical and family history suspecting congenital absence of the permanent teeth .An OPG was taken which showed congenital absence of 15,31,32,33,41,42,43 and tooth # 13 ,14,23 were impacted as seen in Fig[5]. The third molar buds in both the arches were also absent. A complete medical examination was done to rule out any systemic abnormality. Haematological and biochemical findings were found to be within limits.
 | Fig 5. OPG shows absence of the tooth buds for 15,31,32,33,41,42,43, also note the complete absence of third molars buds
|
Based on above findings the case was diagnosed as Idiopathic Non- Syndromic Oligodontia in Permanent Dentition. The line of treatment planned for the above reported case was extraction of mobile deciduous teeth/root stump, orthodontic tooth movement to correct class II malocclusion and a removable partial prosthetic appliance as our patient is in adolescent age group .The patient is to be monitored every six months to determine the need to refit or remake of removable partial prosthetic appliance. Implants are recommended only for missing anterior teeth and fixed prosthesis latter on in life after the complete growth of the jaw bones.
Discussion:
A tooth is said to be congenitally missing if it has not erupted in the oral cavity and is not visible in radiograph.4 When describing the phenomenon of congenitally missing teeth the term most frequently used is Hypodontia.5 Hypodontia is an anomaly that may result in dental malpositioning, periodontal damage, lack of development of maxillary and mandibular bone height and also shows a significant effect on psychological and aesthetic development of an individual.5
Hypodontia and Oligodontia are either isolated /non syndromic or syndromic i.e. associated with some syndrome. In recent years the following definitions have been used :
Hypodontia: 1 to 6 teeth missing (excluding the third molars)
Oligodontia : more than 6 teeth missing (excluding) the third molars
Anodontia :complete absence of teeth5,6
Several factors like hereditary, trauma , infection to the developing tooth bud , overdose of radiation ,systemic conditions like rickets and syphilis ,several intrauterine disturbances, metabolic disorders and idiopathic factors have been proposed as aetiological factors for Oligodontia. It can occur either as a single entity or in association with some syndrome.7
Oligodontia and hypodontia are associated with dental anomalies like delayed formation or eruption of teeth, reduction in tooth size and form , malposition of teeth (ectopic maxillary canines and ectopic eruption of other teeth),infra positioning of primary molars, teeth with short roots , taurodontism , rotation of premolars and or maxillary lateral incisors , enamel hypoplasia , hypo calcification, dentinogenesis imperfect, speech impairment and deep bite all of which can have a physiological and psychosocial impact on the individual.7,8
Dental manifestations are seen in several syndromes along with malformations of other organs:
Isolated cleft lip/palate
Pierre Robin sequence
Van der Woude syndrome
MSX1
Hypohidrotic Ectodremal Dysplasia [EDA or HED]
Ectodactyly - Ectodermal dysplasia - cleft syndrome[EEC]
Cleft lip palate ectodermal dysplasia [CLPED1]
IP, Bloch - Sulzberger syndrome
Hypohidrotic ectodermal dysplasia and immune deficiency [HED-ID]
Oral facial digital syndrome type1[OFD1]
Witkop tooth-nail syndrome
Fried syndrome
Hair-nail-skin-teeth dysplasia
Rieger syndrome
Down's syndrome
Wolf-Hirschorn syndrome
Marshall's syndrome
Hemifacial microsomia and recessive incisor hypodontia 7,8
In this modern world, hypodontia is often encountered by the dental practitioners. Hence the use of OPG is recommended, together with clinical /systemic examination for the detection or confirmation of dental development and coming to the diagnosis of hypodontia / Oligodontia.
In our case we reported seven permanent teeth missing excluding the third molars. The patient was ruled out for being associated with any syndrome and systemic disorder. Thus, congenital lack of more than six permanent teeth without any systemic disorder or syndrome was suggestive of Idiopathic Non Syndromic Oligodontia in Permanent Dentition.
Conclusion:
The missing teeth, abnormal occlusion or altered facial appearance may cause psychological distress in some or all patients. In the above presented case the patient presented with a class II malocclusion which seem more due to a retrognathic mandible than a prognathic maxilla. Now whether the retrognathism of mandible is caused by under development of mandible due to missing tooth buds in anterior region of mandible (since presence/absence of teeth stimulates/retards the growth of jaw bone respectively) or it is a general manifestation in line with the usual class II malocclusion patients need further investigation. Depending upon the extent of the severity, orthodontist teams up with prosthodontist in treating such cases. Thus such cases should be diagnosed at an early stage so that the effect of psychological distress can be minimized.
References:
1. Hartsfield Jr. Acquired and Developmental Disturbances of the teeth and associated oral structures. In: Mc Donald RE, Avery DR, Dean JA, eds. Dentistry for the Child and Adolescent. 8th ed. St Louis: CV Mosby Co; 2004:103-147.
2. Stewart RE, Witkop Jr CJ, Bixler D. The dentition and anomalies of tooth size, form, structure, and eruption. In: Stewart RE, Barber TK, Troutman KC, Wei SHY, eds. Pediatric Dentistry: Scientific Foundations of Clinical Procedures. 1st ed. St Louis: CV Mosby Co; 1982:87-109.
3. Gorlin RJ, Cerrenka J, Moller K, Horribin M, Witcop CJ. Oligodontia, taurodontia and sparse hair growth. Birth defects 1975; II. 2:39.
4. White SC, Pharoah MJ.Oral radiology principles and interpretations. In: White SC (ed). Dental anomalies .St Louis, PA: Mosby, 2000 pp305-306.
5. Arte S. Phenotypic and genotypic features of familial hypodontia . Academic dissertation. Institue of dentistry, University of Helsinki, 2001
6. Silva Meza R. Radiographic assessment of congenitally missing teeth in orthodontic patients. Int J Paediatr Dent 2003; 13:112-116
7. Shipla,Thomas AM and Joshi JL. Idiopathic Oligodontia in Primary Dentition: CaseReport and Review of Literature.J Clin Pediatr Dent 2007; 32(1): 65-68
8. B.Cakur,S.Dagistan and M Bilge .Nonsyndrromic Oligodontia in Permanent Dentition:Three Siblings. The Internet Journal of dental Science.2006 Volume 3 Number 2 |