Introduction
Cryosurgery is the method of deliberate destruction of tissues by controlled cooling. James Arnott (1851) was first to report on the therapeutic use low temperature in malignant disease by means of salt /ice mixture applied to breast neoplasm. The unique properties of cryosurgery were recognized before the turn of this century and since then use of cold and removal of tissue by freezing has been utilized in various field of medicine with an aim of destroying and removing unwanted tissues. Its success has paralled the development of cryosurgical apparatus and its future progress may also reflect the kind of new technologies that are currently being developed.
The oral mucosa is particularly well suited to the application of the cryoprobe because it is moist and does not require a coupling medium. Healing of the oral mucosa after cryotherapy is relatively uncomplicated by infection or pain although swelling is sometimes pronounced.
The study was designed so as to investigate the role of cryosurgery in various mucosal lesions such as leukoplakia, hemangiomas, mucoceles, pannulas, lichenplanus, granulomatous and hyperplastic lesions.
Methods
21 male patients and 13 female patients suffering from different benign and pre-malignant lesions of the maxillofacial region were diagnosed on the basis of detailed history and histopathological examination, wherever required.
Routine laboratory hematological investigations and complete urine examinations were carried out pre-operatively to rule out any systemic disorder. After thorough assessment, the patients were subjected to cryosurgical procedure.
The available apparatus may be classified into open and closed systems. Open systems involve the direct application to superficial lesions .
The three main types of closed system are thermo-electric which operates by Peltier effect, evaporative sytem which depends on controlled evaporation of liquid cryogen and Joule Thompson .Here, the escape of pressurized gas through a narrow orifice results in internal work being performed as the gas expands, leading to the extraction of heat from the local environment. These instruments produce a temperature at the probe surface of about -70 degree centigrade (nitrous oxide). Ascon type of cryosurgical apparatus operating on Joule-Thompson principle was used in this study.
Two cryoprobes were used depending upon the size and location of the lesions. A disc was used for larger surface lesion.
To speed the cooling rate, the probe was precooled before application to the tissues by letting the gas flow through the probe for 5-7 seconds prior to application to the tissues. Once freezing began, the probe was fixed in place by ice formation and was not moved until thaw began. Large lesions were managed by multiple overlapping applications till the entire disease area was frozen.
For mucoceles and lichen planus a single freeze thaw cycle of sixty seconds freeze was applied .For leukoplakias and hemangiomas double freeze thaw cycles of one and a half to two minutes each were employed .For ranulas, double freeze thaw cycle of one and a half minute each was employed.
For granulomatous and fibrous lesions ,the freezing was extended beyond two minutes with double freeze thaw cycle at each session . A slow thaw of 2-5 minutes was observed in all the instances.
For deep lesions, pressure was applied to depress the probe to increase the depth of the ice ball. For superficial lesions either probe was placed gently or slight traction was applied. The lesion after treatment with cryosurgery was left as such and following drugs were prescribed.
A NSAID -Ibuprofen 600mg orally, eight hourly for three days.
A mouthwash to combat the smell of necrotic tissue -Chlorhexidine mouth wash twice daily. A topically applicable local anesthetic such as benzocaine (to be used if required)
Patients were called on 1st,7th, 15th postoperative days for check up with a follow up period of three to six months. Postoperative findings such as pain, swelling, numbness, trismus and any other complications were observed and recorded.
Results:
The distribution of lesions treated with cryosurgery according to the type of lesion and site of occurrence in the oral cavity are shown in Table 1.
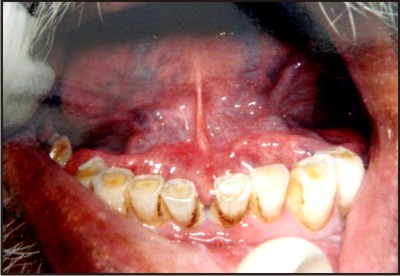
It is evident that all the cases of lichen planus involved the buccal mucosa .Out of the four cases of leukoplakia, two involved the lower lip, one buccal vestibule and one buccal mucosa. All the cases of mucocele except one involved lower lip. One case of mucocele involved the palate. Three cases of pyogenic granuloma involved the maxillary gingiva. Single case of hemangioma involved buccal mucosa. All the four cases of ranula involved floor of mouth (Fig.1)
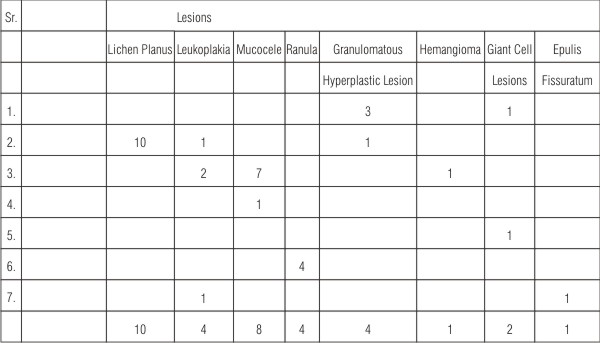 | Table 1 : Distribution Of Lesions Treated With Cryosurgery According To Site
 |
 | Leukoplakia-Pre-Operatively
|
Cryosurgical procedure varied depending on the lesion involved .Cryosurgical procedures includes the following three important aspects:
1. Number of cycles given
2. Duration of each cycle
3. Number of sessions required
It is seen that double freeze thaw cycles of each one and a half minute freeze and 3 minute thaw at overlapping sites were sufficient for all the four cases of leukoplakia and were treated in single session of cryosurgical procedure.(fig.1)
Granulomatous and hyperplastic lesions which included three cases of pyogenic granuloma and one case of fibroma ,required double freeze thaw cycles each of 2 minutes freeze and four minutes thaw. Two sessions of cryosurgical procedure were required for each lesion.
All the lesions of mucocele were treated in single session and each lesion required double freeze-thaw cycle of one minute freeze and two minutes thaw.
Single case of hemangioma required double freeze thaw cycle of one and half minutes freeze and three minutes thaw.
All the cases of lichen planus required double freeze thaw cycle of one and a half minutes freeze and 3 minutes thaw depending upon the size of lesion, the number of sessions required range from two to three.
All the cases of ranula required only a single session. Double freeze thaw cycles of two minutes freeze and four minutes thaw were needed for each lesion (Fig.2)
Two cases of giant cell epulis which were treated with combined surgical and cryosurgical approach required double freeze thaw cycle of two minutes freeze and four minutes thaw.Single session was needed for each lesion.
Single case of epulis fissuratum was given three sessions of cryosurgical procedure consisting of double freeze thaw cycles of 2 minutes each.Lesion was reduced in size but not completely eradicated and had to be treated by surgical excision.
 | Ice ball formed
|
 | Post-Operatively
|
 | Sloughing and necrosis
|
 | Ranula-Pre-Operatively
|
 | Ice Ball Formed
|
 | Post-Operatively
|
Discussion
Cryosurgery is a successful mode of therapy for the conditions which have traditionally presented problems in the management such as leukoplakia,vascular malformation and certain extensive surface lesions like lichen planus.
The technique of freezing has been used to treat hemangiomas by Chapin M.E.et al(1976)1, Hartman p.k.et al (1984)2 and Haim Tal et al (1992)3.
Applications of selected freezing have been employed to treat leukoplakia and hyperkeratosis by Emmings et al(1967), Sako et al(1969),Gongloff r.k.et al (1980)6 and Ishida C.E.(1998)7. With the advancement in cryosurgical technique and equipment,it was utilized in pyogenic granuloma, angioma, fibroma, keratoacanthoma.
Lichen planus was treated with cryotherapy with good results by Sankodi I.(1979)8,Bekke J.P.H.et al(1979),Loitz G.A.(1986) and Ishida.C.E.(1998)7
Cryosurgery was also used to treat trigeminal neuralgia (Barnard J.D.W. et al,1979;Zakrzewska J.M., 1986, 1988,1991)10,s11,12salivary gland neoplasms(Emmings et al,1967)18.
It is concluded from above mentioned studies that within its limitations ,cryosurgery is an effective, simple, predictable, relatively self limiting and safe method for almost all types of oral lesions.As it causes necrosis and sloughing as part of treatment ,delayed healing is an inherent problem with this technique else,it is free from complications such as pain,haemorrhage ,infection,inadvertant damage to adjacent structures ,or scar formation that are seen with knife excision or electrosurgery.
In the present study ,four cases of leukoplakia were treated.Healing was completed by two to three weeks after the last application.No postoperative complications were observed except mild pain and swelling.The results are in conformity with those of Sako et al (1972) ,Poswillo(1974) and Vercellino (1980) who also reported a successful treatment of leukoplakia with cryosurgery.
The management of oral hemangiomas is required in those cases where spontaneous remission do not occur or that occur in older individuals.These lesions are treated by surgery,radiation therapy,sclerosing agents injected into thhe lesions,compression,selective embolization and cryotherapy.Surgical removal is difficult because of uncontrollable haemorrhage during the procedure.Radiation therapy has its own disadvantages such as xerostomia, osteoradionecrosis and malignant changes of benign tissue.
Other modalities such as sclerosing agents and compression require long duration of treatment consisting of multiple injections at 6-8 weeks intervals and even then, results are unpredictable.Selective embolization pose high risks of CVAs. However, cryotherapy appears to be a simple,safe and predictable method of treatment.
In the present study,one case of hemangioma present on buccal mucosa was treated in one sitting with excellent results.These results are in confirmity with those of Poswillo D.E. (1971)15, Sankodi(1979)8, Haim Tal (1992)3 who reported successful treatment of hemangiomas with cryotherapy..W
Mucoceles are benign cystic lesions which frequently occur on lower lip.Trauma to the minor salivary glands play a significant role in etiopathogenesis of these cysts.High rates of recurrence was reported after surgical excision of the lesion.Cryotherapy emerged as a alternative modality in the present study.All the cases except one showed good results with minimum of postoperative complications.One case recurred after one month and was treated by marsupilization.
The treatment of ranula ranges from complex excision of gland to a simple marsuplisation.However,surgery in the floor of the mouth is asssociated with a risk of injury to wharton's duct and to lingual nerve ,profuse bleeding due to rich blood supply and high risk of infetion due to loose areolar tissue in various spaces in this region.All the cases of ranula in this study showed complete ablation .Mild to moderate postoperative pain and swelling was seen.Mild transient paresthesia was reported in one of the cases.Thus cryosurgical procedure is a good preference in the treatment of ranulas.These results are in confirmity with the reports of Marvin E.Chapin (1976)14,who have successfully treated ranulas with cryotherapy.
Lichen planus is basically a skin disease.Mutiple etiological factors have been suggested including infection,trauma,stress,immunologic factors,hypertension and contact allergy to certain metals.It is present in oral cavity in various forms sucreticular, papular, bullus, erosive and plaque like.Many treatment modalities have been proposed for this disease which includes topical steroids,laser therapy,antifungal mouth washes ,surgical excision and cryosurgery.
In the present study, all the patients of lichen planus treated with cryotherapy responded with good results. Pain and burning sensation disappeared with complete healing within four weeks. However, recurrence occurred in two cases, in first case after one year and in the other after 6 months postoperatively. But the period of remission of this troublesome disease was significant. Moreover, cryoapplication can be easily repeated without any harm to patient. Therefore, cryosurgery is a good treatment modality atleast a palliative therapy for oral lesions of lichen planus.
These results are in confirmty with Bekke and Baart(1979)16,Sonkodi(1979)8 who employed cryosurgery to treat lichen planus with good results.
In the hyperplastic and granulomatous lesions , pyogenic granulomas , fibroepithelial polyps, fibromas and some papilloma constitute the most prevalent lesions of the oral cavity. These tumors and tumor like lesions that appear on the tongue ,gingiva, oral vestibule ,floor of mouth and lips are generally the result of inflammatory and hyperplastic reactions to local,chronic irritative factors. Conventional surgical excision and suturing remain the popular treatment of choice of these lesions. In the present study ,three cases of pyogenic granuloma and one case of fibroma showed good results.
Irregular irritative hyperplastic lesions of the sulcus, associated with chronic irritation from denture flanges , can be managed effectively by cryosurgery. Simple excision in these circumstances leads to loss of sulcus depth, which may necessitate a more radical approach to the problem ,such as vestibuloplasty. Necrosis of the hyperplastic tissue may be achieved with minimal alteration of sulcus depth by cryosurgery. Though cryosurgery is a good modality of treatment for epulis fissuratum as it maintains the sulcus depth but it has its limitation.Small lesions can be easily treated but in large lesions, treatment with cryosurgery is very long and not predictable.
Two cases of peripheral giant tumor were treated in the present study with surgical excision and cryotherapy. Cryotherapy included double freeze thaw cycle with 2 minutes freeze. Both cases showed good result. Though peripheral giant cell granuloma has low recurrence rate but the use of cryosurgery ensures the complete eradication of lesion.
With the recent development of better equipment and use of liquid nitrogen, this mode of therapy appears to have promising role in the management of locally aggressive and recurrent lesions. Thus, its simplicity in application and the absence of postoperative infection, contraction, scarring and little or no recurrence makes cryosurgery a highly useful method in treating various conditions of oral cavity.
Refrences
1. Chapin ME. Cryosurgery with nitrous oxide: Report of cases. J. Oral Surg. 1976; 34: 717-21
2. HartmanPK, Verne D and Davis RG. Cryosurgical removal of a large hemangioma. Oral Surg., Oral Med., Oral Path.1984; 58(3):280-82
3. Haim Tal. Cryosurgical treatment of hemangiomas of lip. Oral Surg., Oral Med., Oral Path. 1992; 73:650-54
4. Emmings FG, Mirdza, Georgew G Jr. Freezing the mandible without excision. J. Oral Surg. 1966; 24:145-54
5. Leopard PJ. Cryosurgery and its application to oral surgery. Br. J. Oral Surg.1975; 13: 128-52
6. Gongloff RK, Samit AM, Greene Jr GW, Innco GF Gage AA. Cryosurgical management of benign and dysplastic intraoral lesions. J. Oral Surg. 1980; 38: 671-76
7. Ishida CE, Ramos-e-Silva M. Cryosurgery in oral lesions. Int. J. Dermatol.1998; 37(4): 283-85
8. Sonkodi I. Cryosurgery in Stomato-oncology. Int. J. Oral Surg. 1979; 8: 95-101
9. Loitz GA and O'Leary JP. Erosive lichen planus of tongue treated by oral surgery. J. Oral Maxillofac Surg.1986; 44: 580-82
10. Barnard JDW, Lloyd JW and Glynm CJ. Cryosurgery in the treatment of intractable facial pain. Br. J. Oral Surg.1978-79; 16: 135-42
11. ZakrZewska JM, Nally EF and Flint SR. Cryotherapy in the management of paroxysmal trigeminal neuralgia. J. Maxillofac. Surg.1986; 14: 5-7
12. ZakrZewska JM, Nally EF. The role of cryosurgery(cryoanalgesia) in the management of paroxysmal trigeminal neuralgia .A six year experience. Br. J. Oral Surg.1998; 26(1): 18-25
13. Leopard PJ and poswillo DE. Practical cryosurgery for oral lesions. Br. Dent. J. 1974; 136: 185-96
14. Vercellino V, Magnani G, Goia F, Gandolfo S. Our clinical experience with the cryosurgery of oral lesions of odontostomatologic interest. 1980; 29(4): 252-258
15. Poswillo DE. A comparative study of the effects of electro-surgery and cryosurgery in the management of benign oral lesions. Br. J.Oral Surg.1971; 9: 1-7
16. Bekke JPH and Baart JA. Six years with cryosurgery in the oral cavity. 1979; 8: 251-270
|