INTRODUCTION
Speech is a very sophisticated, autonomous, and unconscious activity. Its production involves neural, muscular, mechanical, aerodynamic, acoustic, and auditory factors. As orodental morphological features influence speech, the dentist should therefore recognize the role of prosthetic treatment on speech activity.
MECHANISM
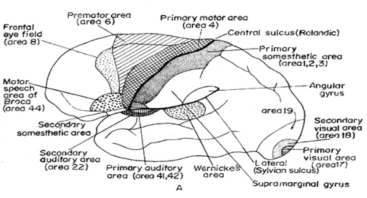
For speech, there are two very important areas in the cerebral cortex,
(i) Broca’s area (after Paul Broca) or area 44,
(ii) Wernickes area (auditory psychic area)
The Broca’s area is situated in the frontal lobe, inferior to the area 4 and the Wernicke’s area in the posterior most part of the superior temporal gyri. In right-handed persons, Broca’s area is found in left frontal (or the dominant hemisphere) lobe.
The mechanism of speech by an example: When someone (A) says “mouse” and the reaction of
another man (B) is as follows, the highest area of hearing gyrus of Heschl (area 41) comes into action. The Wernickes area interpret and understand the word mouse, than broca’s area fire .Which activate appropriates muscles to pronounce the word where.
If the man wants to write what he has seen, the appropriate area 4 will be stimulated from Broca’s area to produce written words on the paper.
Applied physiology
The term aphasia/dysphasia means defective speech due to damage of the Broca’s area, Wernicke’s area. This is due to thrombosis of the feeding artery of the region affected.
Aphasias can be classified as
(I) Sensory,
(ii) Motor, and
(iii) Global
In sensory aphasia, Wernicke’s area is destroyed. The patient hears all right but cannot understand what he is hearing. When he speaks, he cannot understand his own words and the feedback from the ear is lost so there develops some incoherence in the spoken words too. Similarly, there may be failure to understand the meaning of the written words (word blindness).
In motor /expressive aphasia, the Broca’s area is lost. The patient can here and follow spoken words, his internal speech is all right; but when he attempts to express his own thought processes, he fails. In global aphasia there is loss of both Wernicke’s and Broca’s areas
Dysarthria there is a defect in the motor cortex/cerebellum/or basal ganglia, so that vocalisation is imperfect. The term dsyphonia applied to all types of impairment in phonation. An articulatory problem without apparent neurological basis is called dyslalia
Motor process
Respiration provides the raw material for speech. The inspiratory-expiratorv cycle is altered during speech, with a prolongation of the expiratory portion. In phonation the breath stream sets into vibration This breath stream, with periodic and aperiodic component, must be shaped and modified through two additional processes:
1. Resonance, and
2. Articulation
Resonance is the selective amplification of the voiced tone; pharynx, oral cavity, and nasal cavity serves as resonators that reinforce certain components of the tone and suppress others. If the nasal cavities are coupled to the other cavities, a distinctive nasal tone results. The constrictor muscle of the pharynx and the levator palati together accomplish the coupling and uncoupling of these resonance chambers. Such alterations are brought about by differential positioning of the tongue and mandible and by alteration of the orifice through mandibular adjustments and changes in lip opening. Ultimately the breath stream is shaped into sounds (articulation) through impedances produced by various articulators.
Valving Function
Speech is influenced by a series of musculoskeletal valves.
1. Glottal valve- adduction of folds permits the production of a voiced tone and their abduction permits uninterrupted or voiceless passage of air.
2. Palatopharyngeal valve- The muscles of the soft palate and the pharynx constitute palatopharyngeal valve, which couples or uncouples the nasal cavities.
3. linguoavelar valve
4. linguopalatal valve
5. linguoalveolar valve
6. linguodental valve
7. labiodental valve
8. labial valve
The various valves interrupt, impede, and constrict the air stream in many ways to produce the complete repertoire of speech sounds.
COMPENSATORY MECHANISMS
A compensatory mechanism helps the individual to accommodate in startling ways to seemingly insuperable obstacles. Speech is possible even in case of Congenital a glossia or surgical excision of tongue, Children lacking maxillary incisors and yet can produce sounds that depends upon dental impedence of breath, Patients with open palatal clefts- may occlude the cleft, by means of unusual degrees of oral activity and extraordinary tongue movements, and yet produce consonants with an acceptable degree of oral pressure
TYPES OF SOUNDS
Those smallest units which, not carrying meaning themselves, are combined to form the smallest meaningful units of the language—words MORPHEMES, Variable productions of a sound is called ALLOPHONES, recognized as variants of that sound, and they are appropriately grouped into a family, called a PHONEME. The phonemes of English can he divided into four groups: vowels, diphthongs, consonants, and combination
Vowels- Are open voiced sounds, involving vibration of the vocal folds and relatively unimpeded by the oral valves in their egress. (a, e, i, o, u and sometimes y).
Diphthongs- Are blends of two vowels spoken within a single syllable without interruption of phonation.
Consonants- Are phonemes, characterized by considerable impedance of breath stream and used adjacent to vowels and diphthongs to build syllables e.g church, judge, sauce, think, there.
Combination- Is a blend of a consonant and a vowel articulated in such quick succession that they are identified as a single phoneme although the blend can be separated into two-component sounds e.g beauty.
Classification by Place of Production
Labiodental Consonants:
The fricatives /f/ and /v/ are produced by forcing the breath stream through the contact made by the maxillary incisors with the posterior third of the lower lip. In the case of /f/, the breath stream is voiceless; in the case of /v/, the breath stream is voiced. The oral emission of these pressure consonants, the palatopharyngeal valve is closed.
If the upper anterior teeth are too short (set too high up), the v sound will be more like an f. If they are too long (set too far down), the f will sound more like v.
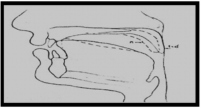
LINGUADENTAL CONSONANTS
The fricatives (e.g., th in this) are produced by forcing the breath stream through the constriction produced when the tip of the tongue is protruded between maxillary and mandibular incisors; the tongue and maxillary incisors touch or are closely approximated. The phoneme /theta/is voiceless and /delta/ voiced. For the oral emission of these pressure consonants, the palatopharyngeal valve is closed.
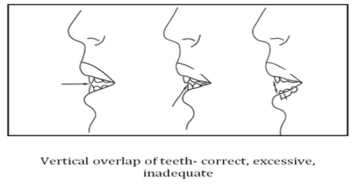
If about 3 mm of the tip of the tongue is not visible, the anterior teeth are probably too far forward (except in patients with a Class II malocclusion), or there may be an excessive vertical overlap that does not allow sufficient space for the tongue to protrude between the anterior teeth. If more than 6 mm of the tongue extends out between the teeth, the teeth are probably too far lingual.
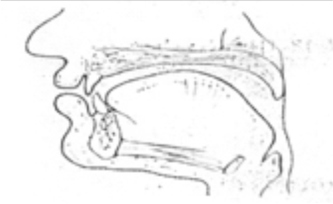
LINGUOLVEOLAR CONSONANTS
The three consonants /t/, /d/, and n have a common articulatry positioning, although two are plosives and one is nasal. The tip of the tongue contacts the alveo1ar ridge, with the sides of the tongue in tight contact with the teeth and gingivae. In the case of /t and /d, the palatopharyngeal valve is closed; impounded breath pressure is suddenly exploded orally.
In the case of /n/ the palatopharyngeal valve is open and the voiced breath stream is emitted nasally
The lingua-alveolar fricatives /s/ and /z/ result from the formation of a narrow midline groove of the tongue through which air is directed against the incisal edge of the teeth. The lateral margins of the tongue contact the teeth and gingivae and the blade of the tongue nearly touches the alveolar ridge. The palatopharyngeal valve is closed and the breath stream is unvoiced for /s/ and voiced for /z/.
The important observation when these sounds are produced is the relationship of the anterior teeth to each other. The upper and lower incisors should approach end to end but not touch. A phrase such as “I went to church to see the judge” will cause the patient to use these critical sounds, and the relative position of the incisal edges will provide a check on the total length of the upper and lower teeth (including their vertical overlap).
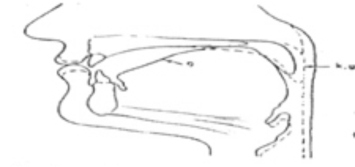
Linguo palatal Consonants
The consonant /r/ is a voiced semivowel; the sides of the tongue touch the maxillary teeth. The tip of the tongue is often pointed to an immediately post-dental area, but at other times, it is the tongue blade that is arched highest toward the palate while the tip points down. The palatopharyngeal valve is closed.
The consonant /j/ is a voiced linguapalatal glide, It is initiated with the tongue raised toward the front of the hard palate but in the course of its production the tongue moves to a position appropriate for articulation of the following phoneme. The palate pharyngeal valve is closed and the teeth are nearly approximated.
LINGUOAVELAR CONSONANTS
The so-called back consonants or gutturals, /k/, /g/. It produced by contact of the middle of the tongue with the soft palate. In the case of the plosives /k/ and /g/, the palatopharyngeal valve is closed; pressure is build up behind the linguavelar contact, and then released. In case of /ng/ (sing) the palatopharyngeal valve is open and the voiced airstream is nasally resonated
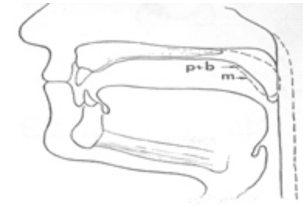
BILABIAL CONSONANTS
Distinctive valving involves the lips: in three, lip closure and in two, lip rounding, for /p/, /b/. and /n/ intraoral breath pressure is impounded behind closed lips palatopharyngeal valve is closed and the impounded air is suddenly exploded orally.
For production of the nasal /m/ the palatopharyngeal valve is open and the voiced air stream is resonated nasally
The consonants /wh/ and /w/ are bilabial glides. They require rounding of the lips, which subsequently move to the appropriate position for the following phoneme. The palatopharyngeal valve is closed. The voiceless /wh/ has a mild fricative component; its cognate is the voiced /w/.
GLOTTAL CONSONANTS
Consonant in which the constriction is at the level of the glottis (the space between the vocal folds) is /h/. The /h/ is an unvoiced fricative produced by the turbulence created when the breath stream passes between the partially approximated vocal folds. Part of the friction is probably created when the air strikes the surfaces of the pharynx and oral cavity. The palatopharyngeal valve is typically closed. Tongue and lip positions do not influence the character of the phoneme.
METHODS FOR SPEECH ANALYSIS
There are two categories: perceptual/acoustic analysis, and kinematic methods for movement analysis.
An acoustic analysis is based on a broadband spectrogram recorded by a sonograph during the uttering of different phrases containing key phrases.
Kinematic analysis includes such methods as ultrasonics, x-ray mapping, cineradiography, optoelectronic articulatory movement tracking, and electropalatography (EPG). None of these methods is, however, aimed for use in routine practice but rather after the failure of conventional means to improve an impaired speech production
PROSTHETIC CONSIDERATIONS
Older complete denture wearers experience greater difficulties in adapting their speech to new prostheses and need longer time to regain their natural speech. A frequent cause is impaired auditory feedback, and therefore a simple auditory test might be useful in such patients to make a proper diagnosis. Speech adaptation to new complete dentures normally takes place within 2 to 4 weeks after insertion. If mal adaptation persists, special measures should be taken by the dentist or by a speech pathologist. When new prostheses have to be made for these patients, certain difficulties in learning new motor acts may delay and obstruct the adaptation.
Consequently, a virtual duplication of the previous denture’s arch form and polished surfaces, especially the palate of maxillary denture, this procedure will frequently solve a problem that may arise due to speech and adaptation difficulties. Variation in thickness and or volume of denture and of the vertical and horizontal dimension of occlusion may result in unpredictable audible changes to the voice. Patient should be informed about possible effects of modified or new denture on their voice2 .
Denture Thickness and Peripheral Outline
One of the reasons for loss of tone and incorrect phonation is the decrease of air volume, and loss of tongue room in the oral cavity resulting from unduly thick denture bases. The periphery of the denture must not be overextended so as to encroach upon the movable tissues, since the depth of the sulci will vary with the movements of the tongue, lips and cheeks during the production of speech sounds. Any interference result in indistinct phonation, especially if the function of the lips is in any way hindered. In the production of the palate lingual sounds, the tongue makes firm contact with the anterior part of the hard palate, and is suddenly drawn downwards, producing an explosive sound; any thickening of the denture base in this region may cause incorrect formation of these sounds.
The palatal rugae and incisive papilla often serve as a “cue”. Because of the lack of palatal texture on the palatal portion of complete denture can impede proper articulation, one solution is to add rugae1. But if the artificial rugae are over-pronounced, or the denture base too thick in this area, the air channel will be obstructed and a noticeable lisp may occur as a result. To produce the Ch and J, Sh sounds if the palate is too thick in the region of the rugae, it may impair the production of these consonants
VERTICAL DIMENSION
The formation of the labials P, B and M require that the lips make contact to check the air stream. With P and B, the lips part quite forcibly so that the resultant sound is produced with an explosive effect, whereas in the M sound lip contact is passive. For this reason M can be used as an aid in obtaining the correct vertical height since a strained appearance during lip contact, or the inability to make contact, indicates that the bite blocks are occluding prematurely.
With the C (soft), S and Z sounds the teeth come very close together, and more especially so in the case of Ch and J; if the vertical dimension is excessive, the dentures will actually make contact as these consonants are formed, and the patient will most likely complain of ‘clicking teeth’.
THE OCCLUSAL PLANE
The labiodentals, F, V and Ph, are produced by the air stream being stopped and explosively released when the lower lip breaks contact with the incisal edges of the upper anterior teeth. If the occlusal plane is set too high the correct positioning of the lower lip may be difficult, if on the other hand the plane is too low, the lip will overlap the labial surfaces of the upper teeth to a greater extent than is required for normal phonation a’ the sound might be affected.
The Antero posterior Position of the Incisors
In setting the upper anterior teeth consideration of their labiopalatal position is necessary for the correct formation of the labiodental F, V and Ph. The inclination angles of central incisors on duplicate maxillary denture were changed from 0¢ª to +30¢ª to -30¢ª. The change in both direction lead to poorer execution of /s/ sound. The labial angulation seem to have greater effect than palatal angulation3. If they are placed too far palatally the contact of the lower lip with the incisal and labial surfaces may be difficult, as the lip will tend to pass outside the teeth: the appearance usually prevents the operator from setting these teeth forward of their natural position.
If the anterior teeth are placed too far back some effect may be noticed on the quality of the palate linguals, S, C (soft), and Z, in which the tip of the tongue makes slight contact with the upper and lower incisors: this will result in a lisp due to the tongue making contact with the teeth prematurely.
THE PPS AREA
Errors of construction in this region involve the vowels I and E -and the palate velar consonants K, G.
A denture which has a thick base in the post-dam area, or that edge finished square instead of tapering, will probably irritate the dorsum of the tongue, impeding speech and possibly producing a feeling of nausea. Indirectly the post-dam seal influences phonation, for if it is inadequate the denture may become unseated during the formation of those sounds having an explosive effect, requiring the sudden repositioning of the tongue to control and stabilize the denture; this applies particularly to singers. Incidentally, speech is usually of poor quality in those individuals whose upper denture has become so loose that it is held in position mainly by means of tongue pressure against the palate.
WIDTH OF DENTAL ARCH
If the teeth are set to an arch which is too narrow the tongue will be cramped, thus affecting the size and shape of the air channel; this results in faulty phonation of such consonants as T, D, S, M, N, K, C and H, where the lateral margins of the tongue make contact with the palatal surfaces of the upper posterior teeth. Every endeavour should be made, consistent with the general mechanical principles, to place the lingual and palatal surfaces of the artificial teeth in the position previously occupied by the natural dentition
Relationship of the Upper Anterior to the Lower Anterior Teeth
The S sound requires near contact of the upper and lower incisors so that the air stream is allowed to escape through a slight opening between the teeth. In abnormal protrusive and retrusive jaw relationships, some difficulty may be experienced in the formation of this sound, and it will probably necessitate adjustment of the upper and lower anterior teeth antero posteriorly, so that approximation can be brought about successfully. The consonants Ch, J and Z require a similar air channel in their formation.
Summary
To summarize, it will be seen that speech requirements call for dentures having a correct vertical dimension, an accurate periphery and an arch formation permitting natural tongue space, so that adequate freedom for movement is ensured. The position of the anterior teeth should be such that they follow that of the natural teeth, thus fixing the occlusal plane at the correct level and preventing the placing of the artificial teeth inside or outside the natural arch, which would require the tongue to adapt itself to new circumstances. Finally, denture bases should be fashioned suitably thin, but consistent with the other factors of denture construction, so that contact by the tongue takes place in as near a natural and normal manner as is possible.
REFERENCES-
1. Christina A.Gitto; a simple method of adding palatal rugae to a complete denture; JPD 1999; 81; 237-9
2. Ebeehard seifert; can dental prosthesis influence vocal parameters; JPD 1999; 81; 579-85
3. Christoph runte; the influence of maxillary central incisor position in complete denture on /s/ sound production; JPD 2001; 85; 485-95
4. Earl pound; utilizing speech to simplify a personalized denture service; JPD; jan 2006; 1-9
5. Chaudhuri; concise medical physiology; 3rd edition; 542-543
6. Jhon J Sharry; complete denture prosthodontics; 126-140
7. HRB fenn; clinical dental prosthetics; 2nd edition; 302-308
8. Zarb bolender; prosthodontic treatment for edentulous patients; Elsevier publication; 12th edition; 379-387 |