|
|
|
| Management Of Microtia In A Low Resource Set Up |
Sajani Ramachandran 1 , Prof Zile Singh 2
1 Assistant Professor, Department of Dentistry - Pondicherry Institute Of Medical Sciences, Pondicherry
2 Prof. & Head Dept Of Community Medicine - Pondicherry Institute Of Medical Sciences, Pondicherry
|
| Address For Correspondence |
Dr. Sajani Ramachandran MDS
Assistant Professor
Department of Dentistry
Pondicherry Institute Of Medical Sciences,
Pondicherry
Email Id : sajaniram@hotmail.com
Phone No : +919894136826 |
| Abstract |
| Microtia, the most common congenital auricular defect can be managed surgically and prosthodontically. A silicon based auricular prosthesis was fabricated at a very low cost for a patient who could not afford expensive treatment but eager to have his defect corrected. |
|
| Keywords |
| Auricular, prosthesis, silicone , low cost prosthesis, microtia |
|
| Full Text |
Introduction:
Auricular defects may be congenital or acquired and they are the second most common craniofacial malformation after cleft lip and cleft palate. The most common congenital auricular defect is microtia. It is a congenital deformity of the pinna, which can be unilateral or bilateral and occurs in about one out of 8,000 - 10,000 births. In unilateral microtia ,the right ear is most typically affected. It is usually associated with atresia of the external auditory canal. The classic occurant usually seen in microtia is comma shaped with upper portion containing a small cartilage [1].
Surgical correction or prosthetic rehabilitation are the two options available for correction of auricular defects.Some patients do not prefer surgical intervention and may not be able to afford the very expensive silicone materials used for prosthetic rehabilitation.Fabrication of a silicone prothesis for a patient who wanted a cost effecticve but aesthetically acceptable prosthesis is described here.
Case History:
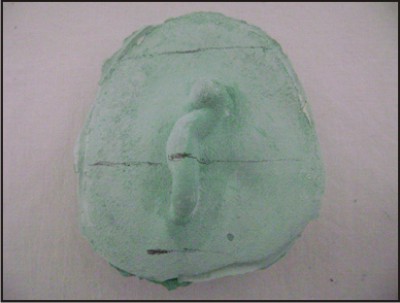
A 23 year old male patient reported to the PIMS ,Pondicherry rural health centre under the community medicine department with a microtia of the left ear (figure 1). The patient, a fisherman by profession wanted to know if the repair could be done with out involving surgery.He had earlier consulted many centres before and was offered surgical
 | Figure1: Unilateral Microtia
 |
correction as option which he could not take because of its prohibitive cost.He was eager to have a prosthetic replacement of the missing parts of the ear but was at the same time concerned about his ability to finance such a procedure.
Challenge:
Apart from the aesthetic and the physical aspect, here, we had to contend with the fact that this patient,as eager as he was to have his defect corrected would be helped only if the prosthesis was done at a bare minimum cost.The fabrication of ear prosthesis is a challenging maxillofacial replacement procedure as it involves dealing with severe undercuts and pronounced convolutions of ear surface. [2]
Clinical Procedure
The area around the ear was outlined with an indelible pencil. Co-ordinates of the vertical and horizontal axes of the ear were made on the patients skin .These marks on the skin were transferred with the impression and was seen on the working cast (figure 2). The co-ordinates helped in proper orientation over the defect while making a new ear form. Impression was made with the patient lying on his side in a supine position. The defect was isolated and the adjacent hair covered with petrolatum.The patients skin was boxed to the circumscribed outline with a collar of wax. Impression was made with irreversible hydrocolloid material
 | Figure2: Working Cast With The Markings Transferred
|
(Alginate,Ruthenium Dental Products Pvt Ltd) with 50% more water to improve its flow properties and facilitate impression procedure. A backing with quick setting plaster (Dental grade plaster of paris,Ramaraju surgical co.Rajapalayam India) was done to provide support to impression. Gauze was used to unite the impression materiel to plaster backing. Material was allowed to set and then removed and was inspected for inaccuracies and working cast was poured. The impression of the contralateral ear was also made similarly and cast was obtained .The impression of donor ear was used to obtain accurate pattern . The advantage of using matching donor ear impressionwas that it has a natural appearance and is time saving.[3]
An individual with similar proportioned ear was selected. Ear mould was created by boxing and impression was made with irreversible hydrocolloid after placing cotton in the external acoustic meatus .Once the impression was obtained, molten modelling wax (Hiflex ,Prevest Dentpro Ltd) was poured into ear mould and solidified wax form was removed and the contour and size was adjusted according to the contralateral ear .Tissue surface of wax form was softened and with the marked co-ordinates it was seated on the defect area of the working cast. The wax pattern was checked for symmetry by placing over the patient's defect site (figure 3). Surface details were applied on the wax pattern. Entire surface was stippled to match the skin texture of the patient.Stippling was made more prominent as some details could be lost during processing. The margins were thinned and blended to the adjacent skin. The residual margin camouflaged the part of the anterior margin .(figure4)
 | Figure3: Wax Pattern Tried On The Patient For Assessing Symmetry
|
 | Figure4: Wax Pattern Contoured To The Working Cast
|
A patch allergy test was done for the patient with the silicon material (multisil RTV, SP Sai Biomed Mumbai, India) and the adhesive(Proskin,Technomed India Pvt Ltd,New Delhi,India) applied on his forearm and the patient was recalled after 48 hours to check for any allergic manifestation. Skin tones were selected with different color tabs made of silicon. The coloring was done by artist's oil color(Camel artist's oil colour, Camlin Ltd,Mumbai,India) using empirical trial and error method.
Processing
The wax ear was invested in a three part mould and after dewaxing ,silicon material was filled in the mould after coloring the material to the appropriate shade.
The processing was done (figure5). The prosthesis was retrieved from the mould and cleaned and was retained by using medical adhesive to the residual tissue present (Figure6). Facial prosthesis may be retained by mechanical means or by using adhesives. Facial prosthetic adhesives are commonly dispensed as pastes, liquids which may be paintable or spray ons and double sided tapes. Studies done earlier have found that prosthetic adhesives have good wettability, fast drying, adhesive to skin, clean off easily and adhesive to silicone[4]. Adhesives require practice and precision of the wearer to obtain correct initial placement of the prosthesis[5]
 | Figure5: Prosthesis After Processing
|
 | Figure6: Prosthesis Retained With An Adhesive
|
Care Of Prosthesis
Patient was advised to keep skin surface clean and free of natural oil secretion to increase proper adhesion of appliance. Removing old adhesive from skin and prosthesis before applying a thin layer of adhesive to periphery of prosthesis should be done . The patient was also given a spectacle in order to camouflage the borders of the prosthesis.
Discussion:
There are 4 grades of microtia
Grade I: A slightly small ear with identifiable structures and a small but present external ear canal.
Grade II: A partial or hemi ear with a closed off or stenotic external ear canal producing a conductive hearing loss.
Grade III: Absence of the external ear with a small peanut vestigeal structure and an absence of the external ear canal and ear drum
Grade IV: Absence of ear or anotia. The most common type is gradeIII.[6]
There are two main treatments possible in microtia-surgical reconstruction or auricular prosthesis.Rehabilitation with a prosthetic ear matched to the contralateral ear provides a better morphologic result.[7]
The surgical reconstruction of ear results in morphology that is less similar to opposite ear because of its complex nature and is considered to be one of the most demanding challenges for a plastic surgeon. Prosthesis fabrication on the other hand is the most conservative method of correcting ear deformity4
The age at which the outer ear surgery can be done depends on the technique. Earliest age at which surgery can be attempted is at 3. The different options for auricular reconstruction are
1. Rib graft reconstruction-since the implant is patients own living cartilage, the ear continues to grow as the child does.This is preferred after age six so that rib is large enough to provide the donor material necessary.
2. Reconstruction of ear using Med por polyethylene plastic implant.
3. Ear prosthesis: .Prosthetic ears appear very realistic and require few minutes of daily care. They are made of silicone which is colored to match the individual color of the skin and attached using adhesives or implants to which magnets or bar clips are used. The optional age to start wearing a prosthesis is 6-9 years.[8]
Now new techniques are being used for creating auricular prosthesis with a computer aided design /manufacture. (CAD-CAM System ).[9]
Conclusion
Inspite of all the latest technologies and techniques being available many of these treatments are unaffordable to most patients .An alternative cost effective but at same time aesthetically acceptable treatment materials are necessary so that many of the patients who do not come forward for treatment can be targeted for rehabilitation.
References:
1. Pos willo D. The pathogenesis of the first and second branchial arch syndrome.Oral surgery ,Oral medicine, Oral pathology,1973; 35: 302-28.
2. Kenneth & Brown ,Fabrication of ear prosthesis. J Prosthet dent 1969 ;21:670-76
3. James C lemmon, Mark S Chambers, Peggy J Wesley and Jack W Martin, Technique for fabricating a mirror image prosthetic ear. J Prosthet dent 1996; 75:292-93.
4. John F wolfardt, Victor Tain, M Gary faulkner, Narasimha Prasad, Mechanical behavior of three maxillo facial prosthetic adhesive system. A pilot project.J Prosthet dent 1992; 68: 943-9.
5. David F Butler ,Gregory G Gion,Ronald R Rapini .Silicone auricular prosthesis.J Am Acad Dermatol,2000;43:687-690.
6. Tanner PB, Mobley SR, External Auricular and facial prosthesis. A collaborative effort of the reconstructive surgeon and anaplastologist Auricular surgery aesthetic and reconstructive facial plastic surgery North Am 2006, 14( 2) :137-145
7. Russel R Wang, carl Andres, hemifacial microsomia and treatment options for auricular replacement, A review of the literature. J prosthet dent 1999,82:197-204
8. John Beumer III, Thomas A Curtis, Mark T , Maxillofacial rehabilitation in prosthodontic and surgical condition. Ishiyako pub; Euro American Inc.1996.
9. Ting Jao, Fuquiang Zhan, Huing ,Design and fabrication of auricular prosthesis by CAD/CAM system ,Int J prosth 2004; 17:460-4 |
|
|
|
|
|
|