|
|
|
| Multiple Bilateral Talon Cusps: A Report Of Three Cases |
Paras Mull J 1 , Syed Nabeel 2 , Usha Hegde 3 , Gazala Danish 4
1 Consultant Endodontist, Oral and Maxillofacial Pathologist - Smile Maker Clinics, Mysore, Karnataka, India
2 Director, Smile Makers Clinic, Oral and Maxillofacial Pathologist - Smile Maker Clinics, Mysore, Karnataka, India
3 Consultant,Oral and Maxillofacial Pathologist - Smile Maker Clinics, Mysore, Karnataka, India
4 Consultant, Oral and Maxillofacial Diagnostician and Radiologist - Smile Maker Clinics, Mysore, Karnataka, India
|
| Address For Correspondence |
Dr. Paras mull J, Consultant Endodontist
Smile Maker Clinics, #187, 2nd Stage, MG Road
2nd Main, Udayagiri, Mysore-570 019 Karnataka.
Phone: +919844453444, 9845106626
Email: drparas.gehlot@gmail.com |
| Abstract |
| Talon cusp is an uncommon dental anomaly presenting as an accessory cusp-like structure projecting from the lingual or facial surface of anterior teeth in both the primary and permanent dentition. It can occur unilaterally or bilaterally. Three cases with multiple bilateral talons cusp in upper anterior teeth in patients of south Indian origin with no apparent association to any syndrome have been presented. The cases presented here were not associated with other dental abnormalities or syndromes. The talons cusp in these cases did not interfere with esthetics or function. Clinical and radiographic characteristics of this developmental anomaly and the modes of treatment are described. Multiple dental anomalies like talons cusp should be reviewed carefully, since they could be a cause of functional and esthetic problems, and could be associated with syndromes. |
|
| Keywords |
| Talon cusp, Accessory cusp, Multiple Talons cusps, Bilateral |
|
| Full Text |
Introduction
The talon cusp is an uncommon dental anomaly manifesting as an accessory cusp-like structure, projecting from the lingual or facial surface of anterior teeth of either dentition.1 It was first described by WH Mitchell in 1892, and was named as "Talon cusp" by Mellor and Ripa in 1970 because of its resemblance in shape to an eagle's talon.2
The etiopathogenesis is multifactorial, and is thought to be polygenetic with some environmental influences. Talon cusp may occur as an isolated entity or in association with syndromes.3,4,5 Hattab et al have classified talon cusp as True talon (Type I), Semitalon (Type II) and Trace talon (Type III), based on the degree of formation and extension.3
Clinically it can pose esthetic and functional problems to the patient.3,6 Talon cusp affects both sexes and commonly is unilateral, but one fifth of the cases are bilateral.7
The objective of this paper is to report three cases with multiple bilateral talons cusp in upper anterior teeth in patients of south Indian origin with no apparent association to any syndrome.
Case Description
Case 1
A 40-year-old male patient reported to our practice with a chief complaint of food lodgement in his upper left back tooth. The patient's medical and family histories were insignificant. Intra-oral examination revealed the presence of proximal caries in maxillary left first molar. Examination also revealed cusp-like projections on palatal surface of maxillary anteriors. The cusp-like structure extended from the cemento-enamel junction to halfway to the incisal edge for central incisors (11,21) and less than halfway for lateral incisors.(12,22) Small tubercle-like projections were seen from the cingula of both the canines.(13,23) (Figure 1) Based on Hattab's classification, maxillary incisors showed Type II talons cusp and the canines Type III talon cusp.
 | Figure 1: Case 1. Intra-oral photograph of maxillary arch showing Type II Talons cusp on four incisors (12,11,21,22) and Type III Talons cusp on both canines (13,23)
 |
Intra-oral periapical radiograph showed a radiopaque V-shaped area superimposing the normal tooth structure, but varying in extension. (Figure 2) Other dental anomalies noted were exaggerated cusp of Carabelli bilaterally.
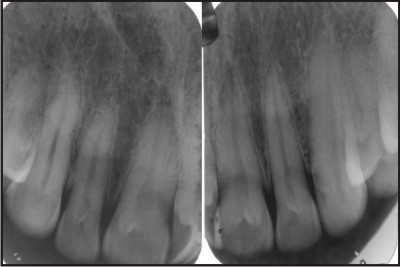 | Figure 2: Case 1. Periapical radiograph of maxillary anterior teeth. Talons cusp reveals as a V-shaped radiopaque structure superimposing over the normal structures.
|
Case 2
A 25-year-old male patient with a complaint of decay in his lower left back tooth reported to our practice. The patient's medical and family histories were insignificant. Intra-oral examination revealed the presence of occlusal caries on mandibular left first molar. Examination also revealed cusp-like projections on palatal surfaces of all maxillary anterior teeth, extending from the cemento-enamel junction to halfway to the incisal edge for central incisors and less than halfway for lateral incisors and canines. (Figure 3) Based on Hattab's classification, maxillary central incisors showed Type II talons cusp and lateral incisors and the canines showed Type III talon cusp. These accessory cusp-like structures did not interfere with esthetic or functional impairment. Intraoral periapical radiograph were similar to the previous case.
 | Figure 3: Case 2. Intra-oral photograph of maxillary arch showing Type II Talons cusp on central incisors (11,21) and Type III Talons cusp on both canines (12,13,22,23)
|
Case 3
A 20-year-old male patient walked in our practice with a complain of discoloured teeth. Medical and family history was non-contributory. Examination revealed brown discoloration due to poor oral hygiene and mild generalised enamel hypoplasia. Examination also revealed cusp-like projections on palatal surfaces of maxillary lateral incisors, extending from the cemento-enamel junction to halfway to the incisal edge. (Figure 4) The accessory cusp-like structures did not interfere with esthetic or functional impairment. Intra-oral periapical radiograph suggested findings similar to the previous cases. The clinical and radiographic features suggested the clinical diagnosis of Type II talons cusp. The talon cusp was associated with caries in relation to right lateral incisor.
 | Figure 4: Case 3. Intra-oral photograph of maxillary arch showing Type II Talons cusp on Lateral incisors (12,22)
|
Discussion
The talon cusp can now be defined as an uncommon dental anomaly manifesting as an accessory cusp-like structure, projecting from the lingual or facial surface of anterior teeth of either dentition.1,8
All reported talon cusps in primary teeth affected the maxillary central incisors, while in the permanent dentition maxillary lateral incisor was most frequently involved (55%), followed by central incisors (33%) and canines (4%).4
Prevalence of less than 1 % to approximaterly 8 % has been reported.4 The variation in talon cusp prevalence could be explained by variation of the condition among different nations, or variation in the samples examined, or examination criteria. 9
The etiology of this anomaly is largely unknown. It may occur as a result of outward folding of the inner enamel epithelial cells (precursors of ameloblasts) and a transient focal hyperplasia of the mesenchymal dental papilla (precursors of odontoblasts).6 Increased localized external pressure on a tooth germ during morphodifferentiation stage may result in either outfolding of the dental lamina as in the case of talon cusp and shoveling or infolding of the lamina as in dens invaginatus.3
Another possible cause of the condition that is discussed is hyperproductivity of the anterior segment of the dental lamina.10 Bilateral distribution of talon cusp in some cases, its association with other dental abnormalities, talon cusp occurring in family members, twins, offsprings from consanguineous marriages and in some genetic syndromes support genetic etiology of the condition.6,7,10
However, sporadic occurrences of this abnormality probably are induced by trauma or other localized insults affecting the tooth germ. Therefore control of the complex processes of dental development appears to be multifactorial. It is primarily polygenetic with some environmental influence.7 Histologically, it is composed of normal enamel and dentin and it may or may not contain pulpal tissue.8
Talons cusp can occur unilaterally or bilaterally. Solitary tooth involvement is the most common finding, but bilateral and multiple involvement is not infrequent.4 One-fifth of the cases showed bilateral distribution of the talon cusp.3 Danker et al found 65% of bilateral occurrence in radiographic study of 15000 anterior teeth.4
There are cases in which both maxillary permanent incisors exhibit this anomaly. In other cases, both lateral incisors or the canines are involved.4 Bilateral talon cusps were seen in 30% of the patients of jordonian population, whereas 70% of those with talon cusps exhibited unilateral talon cusps.9 De Sousa et al. described an unusual case of bilateral talon cusp associated with dens invaginatus.11 Vardhan and shanmugam reported a rare case of bilateral talon cusp on maxillary cental incisors and laterals with dens invaginatus.12 Soares et al reported a case of bilateral bifid talon cusps on the palatal aspect of maxillary permanent incisors.13 Hegde et al reported a very rare case of bilateral labial talon cusps on permanent maxillary central incisors. 14
Sarraf-shirazi et al reported occurrence of multiple talon cusps in three siblings of a family and suggested that genetic inheritance may be a causative factor.15 Talon cusp may present a number of problems both to the patient and the clinician. They include compromised esthetics, occlusal interferences, displacement of affected tooth, carious developmental grooves, pulpal necrosis and periapical pathosis, periodontal problems due to excessive occlusal forces, advanced attrition leading to pulp exposure, irritation of the tongue during speech and mastication, interference with tongue space, problems in breastfeeding, accidental cusp fracture and temporomandibular joint pain. 3,6,13
Treatment may differ depending on each case. Small talon cusps are usually asymptomatic, necessitating no treatment. However, large, prominent and separated talon cusps require definitive treatment with respect to esthetics, occlusion, periodontal and carious problems.3
Deep non-carious grooves and fissures should be cleaned of debris and plaque and prophylactically sealed with fissure sealant. If grooves are carious, the lesion should be eradicated and the cavity filled with glass ionomer restorative material.3
In case of premature contact and occlusal interference, the anomalous cusp should be reduced. If the treatment needs the removal of a substantial portion of the cusp, then reduction should be gradual and on consecutive visits at 6-8 weeks intervals to allow deposition of reparative dentin and pulp obliteration within the extension. Following each grinding procedure, the tooth surface should be treated with a desensitizing agent, preferably fluoride varnish.3,5 However, it is desirable to evaluate and treat the talon cusp soon after eruption to avoid further clinical problems
In all the three cases discussed above the talons cusp did not interfere with esthetic, or functional impairment. However, oral prophylaxis and removal of caries and restoration with Glass ionomer cement was carried out in the taloned teeth in case 3. The patients were made aware of the anomaly and were advised for regular routine follow-up.
Conclusion
Three cases of multiple talon cusps occurring bilaterally have been presented and the clinical implications discussed. Clinical variations of talon cusp include those of location, shape, size, structure and number. Talon cusps occur in a wide variety of world populations and most often are identified in the clinical setting. The importance of recognition of talon cusp lies in the information that it may be useful in identification of syndromes associated with it. Early diagnosis could also result in minimizing the local problems such as, caries, periodontal diseases and malocclusion.
References
1. Siraci E, Cem Gungor H, Taner B, Cehreli ZC. Buccal and palatal talon cusps with pulp extensions on a supernumerary primary tooth. Dentomaxillofac Radiol 2006;35(6):469-72.
2. Mellor JK, Ripa LW. Talon cusp: A clinically significant anomaly. Oral Surg 1970;29:225-28.
3. Hattab FN, Yassin OM, al-Nimri KS. Talon cusp in permanent dentition associated with other dental anomalies: Review of literature and reports of seven cases. ASDC J Dent Child 1996;63(5):368-76.
4. Dankner E, Harari D, Rotstein I. Dens evaginatus of anterior teeth. Literature review and radiographic survey of 15,000 teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1996;81(4):472-75.
5. Abbott PV. Labial and palatal "talon cusps" on the same tooth: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998;85(6):726-30.
6. Hattab FN, Yassin OM, al-Nimri KS. Talon cusp-clinical significance and management: Case reports. Quintessence Int 1995;26(2):115-20.
7. Segura JJ, Jimenez-Rubio A. Talon cusp affecting permanent maxillary lateral incisors in 2 family members. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88(1):90-92.
8. Gungor HC, Altay N, Kaymaz FF. Pulpal tissue in bilateral talon cusps of primary central incisors: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89(2):231-5.
9. Hamasha AA and Safadi RA. Pevelance of talon cusp in Jordanian permanent teeth: a radiographic study. BMC Oral Health 2010;10:6
10. Dumancic J, Kaic Z, Tolj M, Jankovic B. Talon Cusp: A Literature Review and Case Report. Acta Stomatol Croat 2006; 40(2):169-74.
11. de Sousa SM, Tavano SM, Bramante CM. Unusual case of bilateral talon cusp associated with dens invaginatus. Int Endod J 1999;32(6):494-98.
12. Vardhan TH and Subramanyam S . Dens evaginatus and dens invaginatus in all maxillary incisors: Report of a case. Quintessence Int 2010; 41(2): 105-107.
13. Soares AB, de Araujo JJ, de Sousa SM, Veronezi MC. Bilateral talon cusp: Case report. Quintessence Int 2001;32(4):283-86.
14. Hegde KV, Poonacha KS, Sujan SG. Bilateral Labial Talon Cusps on Permanent Maxillary Central Incisors: Report of a Rare Case. Acta Stomatol Croat 2010; 44(2):120-122.
15. Sarraf-shirazi A, Rezaiefar M, Forghani M. A Rare Case of Multiple Talon Cusps in Three Siblings. Braz Dent J 2010; 21(5): 463-466. |
|
|
|
|
|
|