Non retentive unstable swallowed partial dentures when impacted in the oesophagus can be a diagnostic and therapeutic challenge. The incidence of swallowing partial denture is reported in range of 3.6% to 27.7% with adult preponderance1. Other ingested foreign bodies of dental origin are transpalatal arch, a fragment of upper removable appliance, a piece of arch wire and a lower spring retainer2. Controlled prospective studies of impacted denture have not been conducted because of location, size, shape and duration of impaction, experience and availability of flexible and rigid esophagoscope resulting in report of institution or author only3. This study is based on restrospective analysis of 64 cases of denture impaction during a period of 16 years.
Materials And Methods
Over a period of 16 years (JANUARY 1992 to SEPTEMBER 2008), a total of 64 patients with presentation suggestive of swallowed denture were admitted in Cardiothoracic surgery department at university Hospital of BANARAS HINDU UNIVERSITY. Data collection consisted of, sorting out of all these cases of dental impaction from the operation theatre register and analysis of patient files. The records were analyzed for each patient's age, sex, time of ingestion to presentation, presenting symptoms, preceding event, duration of denture wearing, the type of denture (upper, lower, hooked, unhooked), complications, modes of removal and subsequent complications.
All the patients were subjected to routine blood tests, soft tissue X-Ray of the anterior-posterior and lateral neck region, X-Ray of the chest, thin barium or gastrograffin swallow study. Very few required computerized tomographic (CT) Scan for localization. Cases were divided on the basis of site of use (upper or lower denture), the number of teeth present, with hooks made of pointed steel wires, and unhooked dentures. An abnormal cervical or thoracic radiogram consisted of one or many features such as, presence of a radio-opaque denture, widening of the prevertebral space, air in the esophagus, loss of normal lordosis, masking effect of soft tissue mass and free air in tissues consistent with surgical emphysema, and hydropneumothorax. A diagnosis of an impacted denture in the esophagus was made on a combination of history, examination and radiological findings. The age and sex distributions, duration of the use of the denture, events preceding and contributing factors responsible for denture impaction were noted.
Barium study was the investigation of choice, it could outline the site, shape and size of the impacted denture. To some extent, it revealed the degree of tissue damage by showing the tenting of the esophageal mucosa, pressure necrosis with danger of impending rupture, and fistula. In CT Scan the impacted denture with a thickened segment, regional inflammation, localized air space, perforation with air fluid leakage could be identified.
Flexible or rigid hypo-pharyngoscopy, esophagoscopy, and in selected cases panendoscopy including tracheo-bronchoscopy if impaction into trachea was suspected were used for diagnostic and elective therapeutic purpose. Strategy for removal of impacted denture in cervical esophagus was esophagoscopy along with horizontal rotation and vertical traction with a forceps. Dentures removed surgically using synchronous direct manipulation after surgical exposure (oesophagotomy) with the assistance of a forceps, and open surgical removal by cervical oesophagotomy, or right posterolateral thoracotomy. Feeding gastrostomy or jejunostomy was performed in indicated cases with esophageal laceration, edema, severe peri-esophageal inflammation, mediastinitis abscess formation pre-operative pleural empyema, impaction over aberrant subclavian artery with pre-operative massive haemorrhage.
During the evaluation of the data from the study, bivariate analysis was performed and odds ratio for the respective diagnostic, pre operative and postoperative variables along with its 95% confidence interval was calculated. The results were evaluated with significance levels of p < 0.05. The statistical package for social sciences (SPSS) 13.0 windows compatible program was used for statistical analysis as measure of event frequency, the cumulative incidence or risk.
Result
This study revealed accidental swallowing of dentures in 64 cases. which were found impacted in the cricopharyngeal region or the oesophagus. The patients were managed in the department of Cardiothoracic Surgery in the University hospital, over a period of 16 years.
The male to female ratio was 55 (85.9%) : 9(14%), and the age range was 21 years to 78 years (41.3 9.6) with a median age of 53 years. Patients with more than 45 years of age constituted 75.03% of the cases. None of the cases were below 21 years. Only one female patient had dentures due to congenital absence of upper 2 incisors, otherwise all dentures (upper or lower incisors) were used because of loss of teeth due to trauma or infection.
Table 1
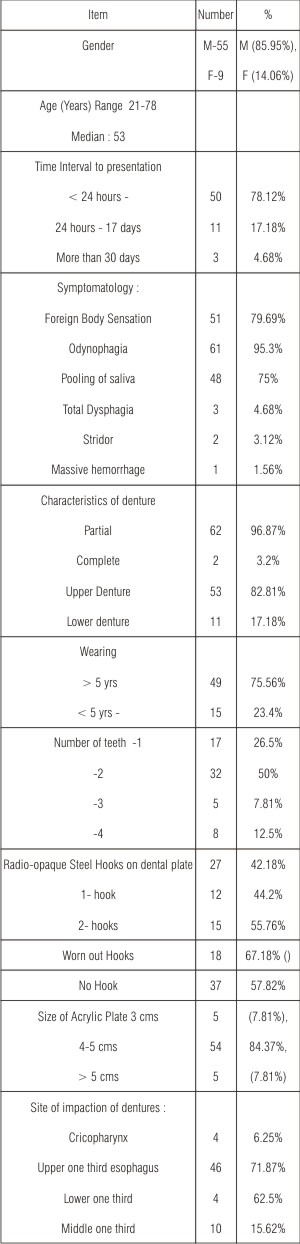 | Table No. 1 Clinical Characteristics of Impacted Partial Dentures Total No. 64
 |
The time interval from accidental swallowing to presentation varied. Fifty patients (78.12%) presented within 24 hours. This was followed by 11 patients (17.18%) presented between 24 hours to 17 days, and the rest 3 (4.68%) presented more than one month after dental impaction, one patient presented 4 years after the incident with massive hemorrhage which later turned out to be hemorrhage from aberrant left subclavian artery. (A setting for dysphagia lusoria)
The symptomatology at the time of presentation was odynophagia in 61 (95.3%), foreign body sensation in 51 (79.6%), pooling of saliva 48 (75%), total dysphagia in 3 (4.68%) and stridor in 2 (3.12%), septicaemia was noticed in 2 (3.12%) lastly massive hemorrhage in 1(1.56%) cases.
The impacted dentures were divided into partial in 62 cases (96.87%) and complete in 2 cases (3.2%), upper incisors' dentures in 53 cases (82.81%) and lower incisors denture in 11 cases (17.18%) (p < 0.01). They were also divided according to steel hooks (clasps) present. In 27 cases (42.18%). Figure 3
One metal hook was present in 12 cases, two hooks were present. In 15 cases, worn out hooks were noted in 18 cases and lastly there were no hooks in 37 cases (57.82%). Figure 2
The number of teeth present in dentures were one in 17 cases (26.5%), two in 32 cases (50%), 3 in 5 cases (7.81%) and 4 in 8 cases (12.5%). The sizes of polymethyl acrylate plates in denture were 3 cms in 5 cases (7.81%), 4-5 cms in 54 cases (84.3%) and more than 5 cms in 5 cases (7.81%).
The sites of impaction of the dentures in this study were pharyngoesophageal junction in 4 (6.25%), upper one third of the oesophagus in 46 (71.87% , p < 0.01), middle one third of the oesophagus in 10 (15.62% p < ns), lower one third of the esophagus in 4 (12.5% p < ns). The patients were wearing the teeth for more than 5 years in 49 (75.56%, z test with correction 3.65 p value < 0.01), and less than 5 years in 15 cases (23.4%).
Table 1
 | Figure No. -2 Extracted dentures without metallic wires
|
 | Figure No. - 3 Extracted dentures with metallic wires
|
The events preceding the impaction of denture revealed elderly people, poor oral sensitivity from dental prosthesis with wrong manner of drinking, or taking medicines in 62 cases (96.37%, RR = 11.2 (CI 95% = 1.9-76.6, p value < 0.0001).
In 19 (29.65%) patients cervical X-Rays were normal and in 14 patients (21.87%) X-Rays of the chest were normal. Table 2
All these patients had dentures identified, and, removed with esophagoscopy or by surgery. In 31 patients (48.43%) an abnormal radio-opaque shadow in cervical X-Ray and in 14 cases (21.87%) abnormal radio-opaque shadow in X-Ray of the chest was detected. In this study, barium swallow study was carried out in 39 cases (60.93%) and CT Scan study was conducted in 7 cases (10.93%). Esophagoscopy was performed in 58 cases (90.62%) with failure of retrieval in 50 (78.12%). No esophagoscopy but direct surgical intervention was done in 5 cases (7.81%) of which 3 (4.68%) had cervical and 2 (3.2%) had thoracic impaction. Table 3
Most of the cases 50 (78.12%) of failure to retrieve had inflammatory reaction with edema, ulceration, tear and food particle impaction. The relative risk of events was > 13 (RR = 13.6; CI 95% = 1.7-74.5); p for tendency < 0.005).
Our strategy for management of impacted denture in the oesophagus was removal. Esophagoscopic removal of impacted denture was by identification followed by direct vertical traction in 3 cases, and identification, disimpaction by horizontal rotation followed by vertical traction with forceps in one case. Left cervical oesophagotomy, disimpaction of the denture and removal was performed in 46 cases (71.87%). In four cases with four teeth synchronous direct manipulation with forceps after exposure was necessary along with gastrostomy in 2 cases and jejunostomy in one case. (p < 0.01). Right posterolateral thoracotomy after prior esophagoscopy, esophageal exploration, identification, esophagotomy and removal of impacted denture was performed in 14 cases (21.87%). Disimpaction with horizontal rotation and removal of impacted denture was performed after carefully observing the reactionary edema, inflammation, ulceration, linear tear, perforation and fistula. Repaired oesophagus was reinforced with pleural flap and intercostals muscle bundle. Temporary gastrostomy was done in 4 cases (6.25%), feeding jejunostomy in 3 cases (4.68%). A Ryles tube was routinely inserted in all surgical cases.
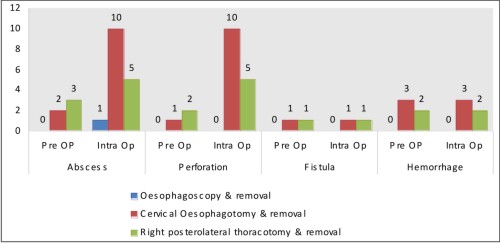
Complications in this series noticed preoperatively and intra operatively caused by sharp impacted denture were abscess in 16 cases (25%), perforation in 15 (23.43%), hemorrhage in 5 cases (7.81%) and fistula in 2 cases (3.12%). Post operative complications were abscess in 5 (7.81%), haemorrhage in 3 (4.68%), perforation in 3 (4.68%) and fistula in one (1.56%). Table 4
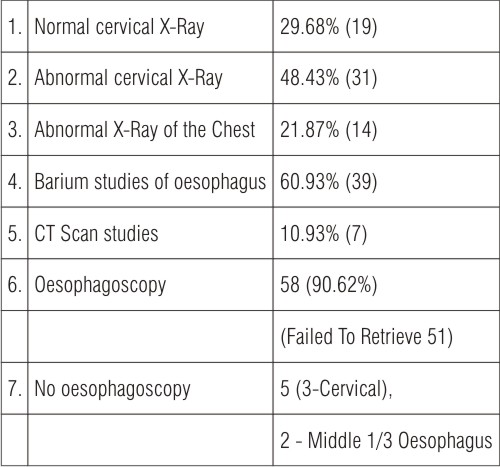 | Table 2 Role of investigations (64)
|
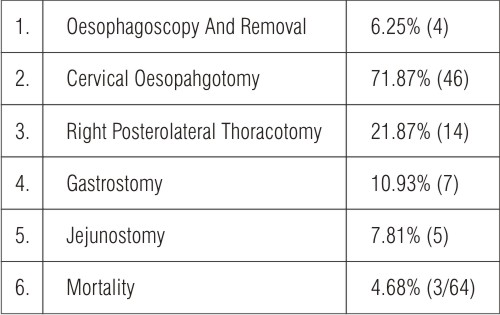 | Table 3 Role of Surgery
|
No statistically significant (p = 0.082) tendency was observed in RR for association between the level of impaction and preoperative complications.
 | Figure No. 4 Closer view of dentures
|
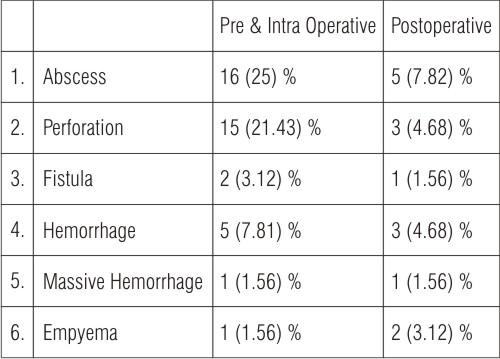 | Table No. 4 Distribution of Complications by percentage
|
 | Figure-1
|
The intra operative abscess, perforation fistulae and haemorrhage were tackled while removal of denture by debridement closure and good haemostasis esophagus was then meticulously closed.
Three deaths (4.68%) occurred in this series. First one due to tracheoesophageal fistula along with pulmonary infection, poor nutrition and septicalmia. The second case was due to esophageal perforation, mediastiinitis mediastinal abscess and erosion of aberrant left subclavian artery. In the third case the mortality occurred after 49 days due to jejunostomy leakage along with peritonitis where the oesophageal denture along with a partially cut snare had been removed. The relative risk of this event did not exceed 1.5, and the 95% confidence intervals comprised the null hypothesis (i.e. RR = 1) therefore corresponding to values of p > 0.05.
Discussion
The phenomenon of the swallowed denture is well documented4,5,6. Dentures are one of the most notorious foreign bodies in the esophagus. Sharp, pointed, serrated edges, metal wire or clasps can lead to damage of the strongest mucosal and submucosal layers of esophagus. This produces direct injury, linear ulceration, compression edema with mucositis, penetration, perforation and fistula7,8.
The occurrence of denture impaction in our study was four per year : Male out numbered the female patients by a ratio of 6 : 1 which was much higher than earlier reported as 3 : 14,10.
Denture made of acrylic material with or without hook wire or clasp and sharp edges (collects) used for more than five year, were not retentive or rugged, and could not readily withstand the forces generated during daily use. Moreover, an upper partial denture without the contact of the lips during drinking could be a predisposing factor or denture impaction. The incidence of upper denture 53 (82.81%) impaction compared to lower denture 11 (17.14%) was significant (p < 0.01) on carrying out a single sample analysis. The incidence of worn out hooks (67.18%) found to be significant (p < 0.05), so was the duration (> 5 years of wearing denture (p < 0.001)4, 9,10.
Symptoms varied from odynophagia (95.3%), foreign body sensation (79.69%) and pooling of saliva (75%) to unusual symptoms like total dysphagia (4.68%) or stridor (3.12%). No hoarseness of voice or respiratory distress could be noted. Neck tenderness was present frequently in cervical impaction. The presence of MACKLER triad (vomiting, chest pain and subcutaneous emphysema) or ANDERSON triad (subcutaneous emphysema, rapid respiration and abdominal rigidity) indicated the suspicion of esophageal perforation11.
The commonest site of the impaction in this study was upper one third of the esophagus to be followed by cricopharyngeal junction and then other sites of anatomical narrowing. Plain radiological imaging could determine the exact site of radio-opaque impacted denture as well as soft tissue edema and air entrapment in cases of penetration, ulceration and perforation but could be of limited value in detecting radiolucent dentures of acrylic resin origin. The radio-opaque wire clasps of the denture could be seen. Barium contrast study of the esophagus performed in 60.93% of cases helped in delineating the denture. Sometimes it was contraindicated due to risk of aspiration. Radio-opaque dentures included barium acrylate, barium fluoride, bismuth glass and barium sulfate and rarely lead foil amalgam. Chest compound tomography was conducted in 10.93% of cases to further locate the denture and condition of the surrounding structures and soft tissues including pneumo-mediastinum, periesophageal fluid collection, extravasated luminal contrast or actual communication of an air filled esophagus and effusion pointing towards perforation. Esophagoscopy was the investigation of choice for evaluating the site, size, mucosal edema, ulceration, impaction, abscess, perforation, fistula and occasionally of therapeutic value. Fluid obscuration, a ridged edematous mucosa, mucosal erosion with impending rupture, bacterial overgrowth and trans location, and systemic sepsis were indications for cervical esopahgotomy or right posterolateral thoracotomy6,12,13. Successful esophagoscopic extraction needed good visualization, use of shear forceps and considerable experience to prevent esophageal perforation which may be up to 23%4. Successful impacted denture extraction by esophagoscopy has been reported to be up to 87% of cases but in our series it was 6.25% only10,14,15.
The indexed series of impacted denture removal by cervical oesophagotomy or right posterolateral thoracotomy was 93% (60 out of 64 cases). This was one of the largest series reported. Routinely, preoperative and post operative endoscopy was performed and a Ryles tube inserted routinely in all cases. Endoscopy performed for surgical cases to check for preceding injuries, to detect size, sharp edges, imbedded hooks or clasps, degree of impaction and to determine the methods of repair or reconstruction9. The surgical removal of impacted denture necessititated cervical esophagotomy or right posterolateral thoracotomy using synchronous direct manipulation including horizontal rotation, disimpaction and removal. Recently, by minimal access surgery with thoracoscopy, small impacted esophageal denture could be removed16.
Delayed treatment of impacted denture in the esopahgus leads to perforation, fistula and necrosis of oesophageal wall and might result in mediastinitis and empyema. Operation at this stage could produce higher incidence of leakage, sepsis and mortality12.
The number of complications found intra operatively caused by impacted denture were more than suspected preoperatively.
Scanning of the complications in this study disclosed pre & intra operative complications abscess (25%), perforation (23.43%), fistula (3.12%) and hemorrhage (7.81%) but Post operative complications were scanty. Abscess (7.81%) perforation (4.65%), hemorrhage (4.68%) and fistula (1.56%). Figure 1
Preoperative complications predisposed to post operative complications. Table 4
Mostly, abscesses, perforations etc were repaired at time of surgery. Only in one patient there was postoperative empyema due repair leak.
Etiology could be attributed to delayed presentation, size of the denture, wavy collets and presence of hooks or clasps. Delayed presentation was associated with excessive edema, longitudinal ulcers, scratched mucosa, penetrated mucosa due to horizontal rotation which precluded safe extraction. Mortality (3 cases) was attributed to mediastinitis, sepsis and in one case hemorrhage from aberrant left subclavian srtery following impacted denture removal
Although this study showed interesting findings, limitations of a methodological nature could not be ignored. Among them were inter observer disagreement and the possibility of error in applicability of the treatment by oesophagoscopic removal and surgical removal. It was very unlikely that the probability of incorrect diagnosis and therapy could have been different (i.e. of differential or non random type) in the group of eventful or uneventful patients. Actually, the existence of a random error would tend to revelence the strength of the association between swallowing of the partial denture and the event they created. Therefore, the real association between swallowing of the partial denture and the subsequent events including complications and mortality might be stronger than found in our study. It was also important to consider that not all patients were examined at the beginning of their swallowing the denture. Thus the validity of the associations was restricted to the premise that the findings during operations represent the condition of the patients at time of presentation. Should these results be generalized with regard to other populations, the local conditions of the study should also be taken into account.
Despite its limitations, the presented results could represent a basis for the development of prospective investigations for a better understanding of the factors related to the prognosis for a patient with partial denture impaction. The duration of impactions, type of symptoms, type, of the denture, age, the level of denture impaction, positive radiographs and complications were the risk factors.
A higher rate of complications with morbidity and occasional mortality could not be used separately for the determination of a therapeutic conduct, a correlation with the clinical data being mandatory.
This study illustrated that prompt management of an impacted denture leads to quick and uneventful recovery. When esophagoscopic removal of impacted denture was not possible, immediate surgical extraction after esophagotomy through cervical or transthoracic route along with disimpaction, horizontal rotation and vertical traction should be performed2,4.
The major lesson learnt from the published literature was that a partial dentures being small were easy target for accidental swallowing and dangerous due to their configuration, dimension and over all rotation in the esophagus. The hazard of small side plate and hook or clasp had long been recognized. The principles of direct and indirect retention and cross arch bracing were important. Medical personnel should be aware of multiple hazards.
Reference
1. TAMURA N, NAKAJIMA T, MATSUMOTO S, OHYAMA T, OHASHI Y. Foreign bodies of dental origin in the air and food passages. Int J Oral Maxullofac Surg 1986; 15 : 739-51.
2. HASHMI S, WALTER J, SMITH W, LATIS S. Swallowed partial dentures. J Royal Soc Med 2004; 97 : 72-5.
3. WILLIAMS EW, CHAMBERS D, ASHMAN H, WILLIAM S, JOHNSON J, SINGH P, MCDONALD AH, REID M, BROWN B. Oesophageal Foreign Bodies at the university hospital of the WEST INDIES. WEST Indian Med J 2005; 54 : 47-51.
4. NWAORGU OG, ONAKOYA PA, SOGEBI OA , KOKONG DD, DOSUM OO. Esophageal impacted dentures. J Natl Med Assoc. 2004; 96: 1350-3.
5. SHIVKUMAR AM, NAIK AS, PRASHANTH KB, HONGAL GI, CHATURVEDY G : Foreign bodies in upper digestive tract. Indian J Otolaryngol and Head and Neck Surgery 2006; 58 : 63-8.
6. CHEN CY, LEE SC, CHEN CW, CHEN JC: Denture Mis swallowing in the sliding esophageal hiatal hernia mimics esophageal perforation. J. Formos Med Assoc 2008; 107 : 663-6.
7. TRESKA TP, SMITH CC. Swallowed Partial denture. Oral Surg Oral Med Oral Pathol 1991; 72 : 756-7.
8. SINGH RK, VARSHNEY S, BIST SS, GUPTA N : An iatrogenic esophageal perforation with denture : How does it happen ? The Internet J Head and Neck Surg 2008; 2 : 2.
9. MORIWAKI Y, SUGIYAMA M, ARATA S, TOYODAH, KOSUGE T, SUZUKI N : Therapeutic strategy for removal of a large dental prosthesis with a sharp clasp, embedded in the esophagus. Endoscopy 2007; 39 : E 303-E304.
10. JASWAL A, JANA AK, HALDAR A, SIKDAR B, JANA U, NANDI TK : Role of prosthodontist with regard to impacted esophageal dentures from an ENT perspective. J Indian Prosthodont Soc. 2007; 7 : 126-31.
11. JOSHI SW, PAWAR A, LAKHKAR D. Denture in esophagus mimicking Carcinoma. Indian J Radiol Imaging 2005; 15 : 229-30.
12. CHUA YKD, SEE JY, TI TK : Oesophageal impacted denture requiring open operation. Singapore Med J 2006; 47 : 820-1.
13. FIRTH AL, MOOR J, GOODYEAR PWA, STRACHAN DR. Dentures may be radiolucent. Emerg Med J 2003; 20 : 562-3.
14. SAMARASAM I, CHANDRAN S, SHUKLA V, MATHEW G. A missing denture's misadventure. Dis Esophagus 2006; 963-5
15. SUTCLIFFE RP, ROHATGI A, FORSHAW MJ, YASON RC. Recurrent laryngeal nerve palsy due to impacted denture plate in the thoracic oesophagus. Case report. World J Emerg Surgery 2007; 2 : 30.
16. PALANIVELU C, RANGARAJAN M, PARTHASARATHI R, SENTHILNATHAN P. Thoracoscopic retrieval of a 'smiling' foreign body from the proximal oesophagus. An impacted denture. Surg Laparoscopy, Endoscopy and Percutaneous Techniques 2008 : 18 : 325-8. |