|
|
|
| Supernumerary Teeth |
Khular Dev Kapil 1 , Wilson Suvil 2 , Arshad Fazil 3 , Hada Singh Yajuvender 4
1 Principal and Head of Department, Department of Conservative and Endodontics - Daswani Dental College and Research Centre, Kota, Rajasthan.
2 Senior Lecturer, Dept of Orthodontics and Dentofacial Orthopedics - Daswani Dental College and Research Centre, Kota, Rajasthan.
3 Senior Lecturer, Department of Oral and Maxillofacial Surgery - Daswani Dental College and Research Centre, Kota, Rajasthan.
4 Senior Lecturer, Department of Conservative and Endodontics - Daswani Dental College and Research Centre, Kota, Rajasthan.
|
| Address For Correspondence |
Dr. Khular Dev Kapil, Principal and HOD,
Department of Conservative and Endodontics,
Daswani Dental College and Research Centre,
Kota, Rajasthan. Ph: 09810809890.
Email Id: khullar_kapil@yahoo.com |
| Abstract |
| Supernumerary teeth are those which develop in addition to the normal teeth. These are an additional entity to the normal series and are seen in all quadrants of the jaw. Supplemental teeth are known as those when these teeth are having normal morphology. They usually don't erupt but are discovered radiographically. Effects of supernumerary teeth on the developing dentition vary. There may be no effect with the supernumerary tooth or teeth discovered either as a chance radiographic finding or following their eruption. Crowding and delayed eruption of adjacent teeth are commonly associated with supernumerary teeth. Surgical removal these teeth are necessary and fixed orthodontic treatment is followed for the space closure |
|
| Keywords |
| Supernumerary Teeth, Mesiodens, Supplemental Teeth. |
|
| Full Text |
Introduction
Supernumerary teeth may be defined as any teeth or tooth substance in excess of the usual configuration of twenty deciduous, and thirty-two permanent teeth1. Supernumerary teeth may occur singly, multiply, unilaterally or bilaterally, and in one or both jaws. Cases involving one or two supernumerary teeth most commonly involve the anterior maxilla, followed by the mandibular premolar region2. Single supernumeraries occur in 76 to 86 percent of cases, double supernumeraries in 12 to 23 percent of cases, and multiple supernumeraries in less than 1 per cent of cases3. Luten's study4 suggests in order of decreasing frequency: upper lateral incisors (50 per cent), mesiodens (36 per cent), upper central incisors (11 per cent), followed by bicuspids (3 per cent). Shapira and Kuftinec5 state the order of decreasing frequency as being: upper central incisors, molars (especially upper molars), premolars, followed by lateral incisors and canines.
Classification of supernumerary teeth may be on the basis of position or form2. Positional variations include mesiodens, paramolars, distomolars and parapremolars. Variations in form consist of conical types, tuberculate types, supplemental teeth and odontomes. Supernumerary teeth may, therefore, vary from a simple odontome, through a conical or tuberculate tooth to a supplemental tooth which closely resembles a normal tooth. Supernumerary teeth are less common in the deciduous dentition with a reported incidence of 0.3 per cent to 1.7 per cent of the population6. Supernumeraries were encountered more frequently in males than females 2,5,7. Multiple supernumerary teeth are more common when a syndrome is involved. Common syndromes showing multiple supernumerary teeth along with other conditions include Gardiner's syndrome, cleidocranial dysostosis, and cleft lip and palate1. Supernumerary teeth most commonly cause diastema, crowding, root resorption of adjacent teeth, malformation of adjacent teeth such as dilaceration, and loss of vitality of adjacent teeth6. Failure of eruption of adjacent permanent teeth is the most frequent occurrence and occurs in 30 to 60 per cent of cases2.
Case Reports
The following cases were referred to the Department of Orthodontics and Dentofacial Orthopedics in Daswani Dental College (Kota) for orthodontic assessment and treatment.
Case 1
A 20-year-old male presented with a chief complaint of unaesthetic smile. Examination revealed a Class I permanent dentition with mesiodens in the maxillary arch. Radiographic examination showed a supernumerary tooth between 11 and 21. (Fig. 1 a,b). The supernumerary tooth was extracted and Orthodontic treatment was used to align the maxillary incisors. The patient is now under regular review after fixed orthodontic treatment.
 | Figure 1 A : Occlusal And Radiographic View
 |
 | Figure 1 B:- Occlusal And Radiographic View
|
Case 2
A 23-year-old male presented with a chief complaint relating to aesthetic concerns regarding his proclined teeth. Examination revealed a Class I malocclusion with bimaxillary protrusion. Radiographic examination revealed the presence of supplemental premolars in lower left quadrant (Fig. 2). Treatment involved the extraction of upper and lower first premolar teeth, extraction of the supernumerary tooth and upper and lower full arch banding to correct the malocclusion.
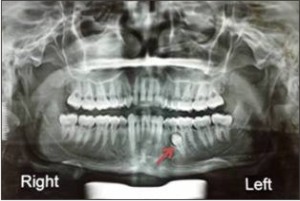 | Figure 2: Radiographic View
|
Discussion
The cases described above represent a small sample of the possible presentations for cases involving supernumerary teeth. It is essential to enumerate and identify the teeth present clinically and radiographically before a definitive diagnosis and treatment plan can be formulated. Not all situations lend themselves to ideal treatment results. Timing of interceptive treatment should be as soon as possible following clinical detection of an abnormal eruption pattern. It has been suggested that a tooth delayed in its eruption by more than six months with respect to its antimere should be radiographically investigated8. A panoramic radiograph is a most useful screening radiograph in such situations as it shows all areas of the maxilla and mandible. Mitchell and Bennett9 have suggested that different types of supernumeraries have been associated with different effects on the adjacent dentition. Foster and Taylor10 examined this relationship and found tuberculate types more commonly produced delayed eruption, whereas conical types more commonly produced displacement of the adjacent dentition.
The options include removal of the supernumerary only, removal of the supernumerary and orthodontic treatment to re-establish sufficient space for the delayed tooth, with or without surgical exposure of the unerupted tooth at the time of supernumerary tooth removal8.
Mitchell and Bennett9 studied spontaneous eruption following supernumerary removal only. Ninety-six patients with 120 teeth exhibiting delayed eruption were studied. They found that 78 per cent spontaneously erupted with a median time for eruption of 16 months. Only 14 per cent required a second operation to expose the delayed tooth and this procedure was performed at a median time of 30 months following supernumerary removal. If adequate space was available, or was created early, the median time for spontaneous eruption was reduced. Timing of surgical removal of supernumerary teeth has also been contentious. Hogstrum and Andersson7 suggested two alternatives exist. The first option involves removal of the supernumerary as soon as it has been diagnosed. This could create dental phobia problems for a young child and has been said to cause devitalization or deformation of adjacent teeth. Secondly, the supernumerary could be left until root development of the adjacent teeth is complete. The potential disadvantages associated with this deferred surgical plan include; loss of eruptive force of adjacent teeth, loss of space and crowding of the affected arch, and possible midline shifts. In their study 23 children aged less than 11 years and 17 aged greater than 11 years at the time of supernumerary removal, Hogstrum and Andersson7 found no evidence of root resorption, loss of vitality or disturbance of root development during the three-year follow-up period.
Conclusion
The position, size and nature of the supernumerary teeth and the level of co-operation of the patient will influence the surgical difficulty. From the evidence available it would seem prudent to treat by removal of the supernumerary teeth only in cases where adequate space is available for the adjacent permanent tooth to erupt. The space should be monitored to ensure that it does not close, and the delayed tooth should be given approximately 18 months to spontaneously erupt. In cases where the delayed tooth is displaced, or where further early orthodontic treatment is indicated, concomitant exposure and orthodontic traction may be considered. In young patients who are unlikely to cope well with a second operation, initial exposure and orthodontic traction at the time of supernumerary removal may be advisable, particularly when incisors are involved.
References
1. Schulze C. Developmental abnormalities of the teeth and jaws. In: Gorlin RJ, Goldman HM, eds. Thoma's oral pathology. St Louis: CV Mosby, 1970:112-22.
2. Mitchell L. Supernumerary teeth. Dental Update 1989; 16:65-9.
3. Solly. Unusual supernumerary teeth. Angle Orthod 1990; 60:289-92.
4. Luten JR, Jnr. The prevalence of supernumerary teeth in primary and mixed dentitions. J Dent Child 1967; 34:48-9.
5. Shapira Y, Kuftinec MM. Multiple supernumerary teeth: report of two cases. Am J Dent 1989; 2:28-30.
6. Taylor GS. Characteristics of supernumerary teeth in the primary and permanent dentitions. Dent Pract Dent Rec 1972; 22:203-8.
7. Hogstrum A, Andersson L. Complications related to surgical removal of anterior supernumerary teeth in children. J Dent Child 1987; 54:341-3.
8. Becker A, Bimstein E, Shteyer A. Interdisciplinary treatment of multiple unerupted supernumerary teeth: a case report. Am J Orthod 1982; 81:417-22.
9. Mitchell L, Bennett TG. Supernumerary teeth causing delayed eruption - a retrospective study. Br J Orthod 1992; 19:41-6.
10. Foster TD, Taylor GS. Characteristics of supernumerary teeth in the upper incisor region. Dent Pract 1969; 20:8-12.
|
|
|
|
|
|
|