Introduction
Extensive review has been carried out in recent years regarding the unusual anatomy of permanent maxillary first molar.Knowledge of the most common anatomiccharacteristics and their possible variations is fundamental, becausethe nontreatment of even one canal can lead to endodontic treatmentfailure.1 The usual root canal anatomy of maxillary first molars has been described as three roots with three canals, with the commonest variation being the presence of a second mesiobuccal canal showing an incidence between 18% and96.1%.2 Case reports with fiveandsix root canals or canals with a C-shaped configurationhave also been reportedearlier.3 4 5 Maggiore et alreported the maxillary first molar having six canals with two mesiobuccal,three palatal, and one distobuccal.6 The occurrence of 2 canals in DB roots has been less frequent andhas been reported in 3.6% of maxillary molars.7 Martinez-Bernaand Ruiz-Badanellireported 3 cases in which the maxillary first molars had presented6 root canals (3 in mesiobuccal, 2 in distobuccal, and 1 in palatine root).8 Adanir reported six canalswith one mesiobuccal, two mesiopalatal, two distobuccal, and one palatal.9 Alavi et aland Thomas et al reported the incidence of two canals in the distobuccalroot as 1.90% and 4.30%, respectively.10 11 Filho et al reported a maxillary first molar with three roots and seven root canals. Ofthe 140 extracted maxillary first molars, only one tooth showed seven root canals in which three mesiobuccal canals, three distobuccal canals, and one palatal canal were identified. Variations in number of palatal root canals have been reported by Christie et al who reported 16 cases of maxillary molars with twopalatal roots found during 40 years of daily clinical practice.12 Currently, technological advances have witnessed the introduction of cone beam computed tomography (CBCT) systemto facilitate the assessment of internal anatomic variations of root canals. This system has been very useful in particular endodontic problemsas a result of identification of anatomic features and variations of the root canal system,because endodontic diagnosis and treatment planning have been difficult to handle with2-dimensional radiographs.13 14
The Present case report discusses the successful endodontic management of a maxillary first molar presenting with three roots and six root canals. This unusual morphology wasconfirmed with the help of cone beam computerized tomography (CBCT) scans.
Case Report:
A 19 year old female patient reported to the Department of Conservative Dentistry, Institute of Dental Studies and with pain in the upper right maxillary first molar for the past two days. The pain intensified during any thermal stimuli and upon mastication. The patients medical history was noncontributory.
Detailed clinical examination revealed a carious ( mesio-occlusal) maxillary right upper first molar which was tender to percussion. Periodontal assessment revealed the tooth was within the normal physiological limits. Heat test using gutta percha stick revealed a lingering pain after the removal of the stimulus. The heat test was first performed on the contra lateral tooth and then on the adjacent tooth.
A preoperative radiograph in relation to the involved tooth revealed deep caries in the mesi-occlusal portion of the tooth involving the pulp space with periodontal ligament space widening in relation to mesiobuccal root ( Fig 1)
 | Fig 1 : Pre Operative X Ray Depicting Mesioocclusal Caries Involving The Pulp
 |
A detailed review of the clinical and radiographic findings led to the diagnosis of acute irreversible pulpitis with acute apical periodontitis. Endodontic treatment was suggested and the procedure was explained to the patient.
The tooth was anesthetized with1.8 mL (30 mg) 2% lignocaine containing 1:200,000 epinephrine (Xylocaine; AstraZeneca Pharma Ind Ltd, Bangalore, India.) followed by rubber dam isolation. An endodontic access cavity was established. Clinical examination with a DG-16 endodontic explorer (Hu-Friedy,Chicago, IL) revealed two canal openings in each of the, mesiobuccal, and palatal root and one opening in the distobuccal root. During the further examination using surgical loupes a second canal was suspected in the distobuccal orifice.
The working length was determined with the help of an apex locator ( Tri Auto ZX, J Morita, Tokyo, Japan) and later confirmed using a radiograph. Multiple working length radiographs were taken at different angulations (Fig 2 )
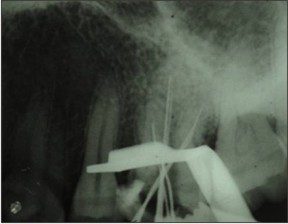 | Fig 2 : Working Length Showing The Files In All The 6 Canals.
|
To confirm the unusual morphology it was decided to obtain a CBCT image of the tooth. An interim dressing of Cavit( 3M , ESPE) was placed and after an informed consent of the patient the CBCT image of the maxilla was performed. The images clearly revealed 6 canals, two in each of the mesiobuccal, distobuccal and palatal roots.
As it can be clearly seen from the image( Fig 3 ) there there were 6 separate canals confirmed with the CBCT imaging. An intraoral photograph was also taken ( Fig 4 )
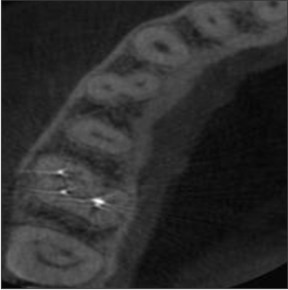 | Fig 3 : Cbct Image Showing 6 Separate Canals
|
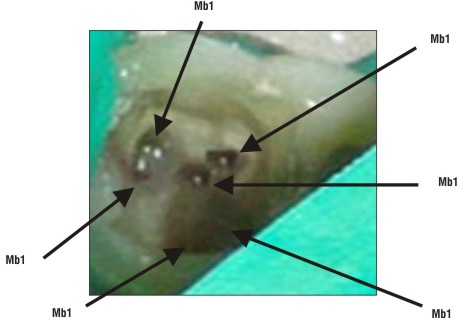 | Fig 4 : Intra Oral Image Showing All The 6 Canals
|
Pulp extirpation was completed in all the canals and an interim dressing of Cavit ( 3M ESPE) was placed in the canals.
In the subsequent appointment the tooth was asymptomatic. Cleaning and shaping of the canals were performed under rubber dam isolation using Protaper Nickel titanium rotary instruments with a crown down technique till file no. F2. Irrigation of the canals were done between each instrumentation using 2.5% NaOCl and 17% EDTA. Normal saline was used as the final irrigant.
The canals were subsequently dried with absorbent paper points and obturated using the F2 ProTaper cone and ZnOE sealer ( Fig 5). The tooth was then restored with a posterior composite Synergy D6 ( Coltene Whaledent). The patient was advised a full coverage restoration.
 | Fig 5 : Obturation X Ray
|
Discussion
A variety of study methods such as radiographs, magnification, clinical evaluations, dye injection,tooth sectioning, and scanning electron microscopy have been discussed and reported by several authors for the prevalence of additional root canals.14 Newer diagnostic methods such as computerized axial tomography (CT) scanning greatly facilitate access to the internal root canal morphology by allowing the operator to look at multiple slices of tooth roots and their root canal systems.15 WithCT scans, it is possible to reconstruct overlapping structures at arbitraryintervals, and, thus, the ability to resolve small subjects isincreased. Additional advantage is thedrastic reduction in scan time and effectivedosages, but they still are not as accurate and do not limit the dosageas low as reasonably achievable.16
The use of newer diagnostic imaging modality (CBCT) is fast gaining importance in diagnosis of unusual root canal morphology as the amount of informationgained from conventional radiographs and digitally captured periapicalradiographs is limited by the fact that the three-dimensional anatomy ofthe area being radiographed is compressed into a two-dimensionalimage.15 CBCT has been used in endodontics for the effective evaluation of theroot canal morphology alongwith the diagnosis of endodontic pathosis, assessing root and alveolarfractures, analysis of resorptive lesions, identification of pathosis ofnonendodontic origin, and presurgical assessment before root-end surgery.17 18 19
The present case report emphasises on the use of CBCT for the identification of multiple root canals and subsequent success of the root canal treatment.
Matherne et al in a studyconcluded thatCBCT images always resulted in the identification of greater numberof root canal systems than digital images.20 Baratto Filho et alevaluatedthe internal morphology of maxillary first molars by ex vivo andclinical assessments and concluded that CBCT scanning along with the use of operating microscope can be used as a good method for initial identification of maxillary firstmolar internal morphology.14 In a study by Jojo Kottoor et al, CBCT axial imagesconfirmed the presence of three roots and seven root canals, namelymesiobuccal1 (MB1), mesiobuccal2 (MB2), mesiobuccal3 (MB3),distobuccal1 (DB1), distobuccal2 (DB2), mesiopalatal (MP) and distopalatal(DP).21
Conclusion
This case report clearly ascertains the use of advanced imaging techniques like CBCT for successful endodontic treatment.
References
1. João Vicente Baroni Barbizam, Rodrigo Gonçalves Ribeiro.Unusual Anatomy of Permanent Maxillary Molars. J Endod Vol. 30, No. 9, September 2004.
2. Kulild JC, Peters DD. Incidence and configuration of canal systems in the mesiobuccal root of maxillary first and second molars. J Endod 1990;16:311–7.
3. Ferguson DB, Kjar KS, Hartwell GR. Three canals in the mesiobuccal root of a maxillaryfirst molar: a case report. J Endod 2005;31:400–2.
4. de Almeida-Gomes F, Maniglia-Ferreira C, Carvalho de Sousa B, et al. Six root canalsin maxillary first molar. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e157–9.
5. Dankner E, Friedman S, Stabholz A. Bilateral C shape configuration in maxillary firstmolars. J Endod 1990;16:601–3.
6. Maggiore F, Jou YT, Kim S. A six-canal maxillary first molar: case report. Int Endod J 2002;35:486–91.
7. Pineda F, Kutler Y. Mesiodistal and buccolingual roentgenographic investigation of 7275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101–10.
8. Martinez-Berna´ A, Ruiz-Badanelli P. Maxillary first molars with six canals. J Endod 1983;9:375–80.
9. Adanir N. An unusual maxillary first molar with four roots and six canals: a casereport. Aust Dent J 2007;52:333–5.
10. Alavi AM, Opasanon A, Ng YL, et al. Root and canal morphology of Thai maxillarymolars. Int Endod J 2002;35:478–85.
11. Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent firstmolar teeth at various ages. Int Endod J 1993;26:257–67.
12. Christie WH, Peikoff MD, Fogel HM. Maxillary molars with two palatal roots: a retrospective clinical study. J Endod 1991;17:80–4.
13. Cotton TP, Geisler TM, Holden DT, Schwartz SA, Schindler WG. Endodontic applicationsof cone-beam volumetric tomography. J Endod 2007;33:1121–32.
14. Flares Baratto Filho, Suellen Zaitter. Analysis of the Internal Anatomy of Maxillary First Molarsby Using Different Methods. JOE — Volume 35, Number 3, March 2009.
15. Patel S, Dawood A, Whaites E, et al. New dimensions in endodontic imaging: part 1.Conventional and alternative radiographic systems. Int Endod J 2009;42:447–62.
16. Kalender WA, Siessler W, Koltz E, et al. Spiral volumetric CT with single-breadth-holdtechnique, continuous transport and continuous scanner rotation. Radiology 1990; 173:567–8.
17. Patel S, Dawood A, Ford TP, et al. The potential applications of cone beam computedtomography in the management of endodontic problems. Int Endod J 2007;40:818–30.
18. Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod2007;33:1–6.
19. Cotton TP, Geisler TM, Holden DT, et al. Endodontic applications of cone-beamvolumetric tomography. J Endod 2007;33:1121–32.
20. Matherne RP, Angelopoulos C, Kulild JC, et al. Use of cone-beam computed tomographyto identify root canal systems in vitro. J Endod 2008;34:87–9.
21. Jojo Kottoor, Natanasabapathy Velmurugan. Maxillary First Molar with Seven Root Canals Diagnosed with CBCT. J Endod 2010;-:1–7 |